When crack use stops, the first hours can feel chaotic. A person may look exhausted but unable to settle, intensely sad but also agitated, hungry but nauseated by the situation they're in, and desperate to use again even when they've already decided they want help. Families often misread this as stubbornness, manipulation, or a simple comedown. It isn't.
Crack withdrawal symptoms follow a recognizable pattern. They're driven by abrupt changes in brain chemistry after repeated stimulant exposure, and they can become dangerous when depression, paranoia, or impulsive behavior take over. The good news is that withdrawal is treatable, and a structured detox setting can make the process safer, calmer, and far more manageable.
Understanding the Initial Crack Withdrawal Crash
The crash often starts before a person has fully processed that the high is over. One moment they're restless and searching for more. Soon after, they may become withdrawn, suspicious, exhausted, irritable, or emotionally flat. Some sleep for long stretches. Others can't sleep at all. Family members sometimes see rapid mood swings and don't know whether to comfort the person, confront them, or call for help.
What the crash actually is
The crash is the first stage of withdrawal, not just a rough comedown. Acute withdrawal can begin within 30 minutes to 72 hours after the last use, and this crash phase is tied to dopamine receptor downregulation, which shows up as severe dysphoria, extreme fatigue, and intense cravings. The phase typically peaks at 24 to 72 hours, and paranoia or hallucinations can appear during that window, according to clinical guidance on crack withdrawal timing and symptoms.
That neurochemistry matters. Crack produces a rapid surge in reward signaling. When use stops, the brain doesn't immediately return to balance. The person isn't “failing to cope.” Their reward system is abruptly underpowered, while stress signaling can feel overactive. That mismatch helps explain why they may look physically drained and emotionally panicked at the same time.
What families usually notice first
A concerned spouse, parent, or partner often reports a cluster of signs rather than one dramatic symptom:
- Sudden exhaustion that looks out of proportion to recent activity
- Irritability or agitation that flares over minor issues
- Suspicion or fearfulness that can slide into paranoia
- A powerful urge to use again to stop the emotional drop
- Sleep disruption in either direction, too much sleep or very poor sleep
The first day doesn't tell the whole story. A person can look quieter after the high fades and still be entering the most unstable part of withdrawal.
This is one reason home detox so often goes badly. Families expect rest to fix it. Instead, craving, low mood, and confusion can intensify. If there's uncertainty about how recent use may affect the next steps, practical context about how long cocaine stays in the system and what influences detection times can also help families understand why symptoms and testing don't always line up neatly.
What works and what doesn't
What helps in the crash phase is calm structure, low stimulation, hydration, observation, and quick access to clinical support if the person becomes unsafe. What doesn't help is arguing, shaming, or expecting promises to override neurochemical distress. During the crash, judgment is often poor. That's why supervision matters early, not only after things spiral.
The Complete Crack Withdrawal Timeline
One of the most stabilizing things for families is learning that crack withdrawal symptoms usually move in phases. The exact experience varies, but the pattern is recognizable enough that clinicians can plan for it. That matters because people tend to panic when symptoms shift. They assume something new is wrong, when in many cases the person is moving into the next stage.
Crack withdrawal timeline at a glance
| Phase | Typical Duration | Common Symptoms |
|---|---|---|
| Crash | 24 to 72 hours | Severe fatigue, cravings, paranoia, hallucinations, body aches |
| Acute withdrawal | 2 to 7 days | Extreme fatigue, trouble sleeping, low motivation |
| Subacute withdrawal | 7 to 14 days | Intense cravings, depression |
| Post-acute withdrawal | 14 to 28 days | Minor cravings, mood fluctuations |
According to clinical research on the crack withdrawal timeline, withdrawal progresses through the initial crash from 24 to 72 hours, acute withdrawal from 2 to 7 days, subacute withdrawal from 7 to 14 days, and post-acute withdrawal from 14 to 28 days. That same source notes that acute symptoms often resolve within 5 days, while less severe symptoms can continue for 2 weeks or more, with mood returning to baseline in about 1 month.
How the stages tend to feel
The crash is abrupt. Energy drops hard, mood crashes, and the person may seem physically spent but mentally unsettled. This is often when families first realize the situation is more serious than they thought.
The acute phase usually feels heavy and flat. A person may struggle to get out of bed, think clearly, or sleep normally. They may say they feel empty, bored, or unable to care about anything.
The subacute phase can be deceptive. Outwardly, the person may appear less chaotic. Internally, cravings and depression can become more obvious because the shock of the first few days has passed.
The post-acute phase tends to be less intense but more frustrating. Mood can swing. Motivation can come and go. Small triggers can feel larger than they should.
Practical rule: Don't measure progress only by whether someone looks calmer. In stimulant withdrawal, a quieter presentation can still include strong cravings and serious depression.
Why a timeline helps
A timeline doesn't predict every symptom. It does reduce unnecessary confusion. It helps families know when to increase supervision, when not to overreact to expected discomfort, and when not to underestimate a sudden emotional downturn.
It also changes expectations. Many people think that once the drug is out of the body, the crisis is over. For crack withdrawal symptoms, the larger struggle is often psychological and continues after the first wave of physical exhaustion begins to ease.
Navigating Physical and Psychological Symptoms
Crack withdrawal symptoms are often misunderstood because the psychological side can be more severe than the physical side. Families may look for dramatic medical signs and miss the symptoms that drive relapse and self-harm risk. The person may not be writhing in pain, but they may still be in a dangerous state.

The symptoms that hit hardest
According to medical guidance on crack withdrawal and detox, crack withdrawal symptoms are predominantly psychological. The most common and persistent symptom is intense craving, followed by profound depression, severe anxiety, anhedonia, paranoia, and difficulty concentrating. In severe cases, suicidal ideation can occur.
That list explains a lot of the behavior families witness. A person in withdrawal may not say, “My dopamine system is depleted and I can't access pleasure.” They may say, “Nothing matters,” “I can't think,” “I'm crawling out of my skin,” or “I just need one hit so this stops.”
Why the brain feels so wrong
Anhedonia is one of the clearest examples of the “why” behind withdrawal. It means an inability to feel pleasure. Food doesn't feel rewarding. Conversation feels flat. Music doesn't help. Rest doesn't refresh. This isn't a character flaw or laziness. It's a predictable consequence of a reward system trying to function after repeated overstimulation.
Common physical complaints can include fatigue, body aches, appetite changes, and sleep disruption. These symptoms are real, but they often become most difficult when combined with anxiety and dread. For families trying to distinguish panic from a medical emergency, a plain-language review of physical symptoms of anxiety can be a useful companion resource.
What symptoms usually mean in practice
- Cravings often need active interruption. Isolation and willpower alone usually aren't enough.
- Depression during withdrawal can become severe quickly. It should never be brushed off as temporary drama.
- Anxiety and paranoia can make the person mistrust helpers, refuse care, or misread neutral situations as threatening.
- Poor concentration affects everything from simple conversations to treatment consent and safety planning.
- Sleep disturbance can worsen every other symptom, especially irritability and impulsivity.
“I know they said they want help” is not a safety plan. Withdrawal can change what a person says and does from hour to hour.
What tends to work best
The most effective response combines observation, emotional de-escalation, and professional care. Short, calm communication works better than long lectures. Reduced stimulation works better than confrontation. Structured treatment works better than promises made during a craving wave.
What usually fails is expecting insight to carry the person through. In stimulant withdrawal, insight and impulse control often don't rise together.
Recognizing Dangerous Withdrawal Signs
Most crack withdrawal symptoms are intensely uncomfortable. Some are dangerous enough to require immediate action. Families need a simple dividing line, because waiting too long can put everyone at risk.
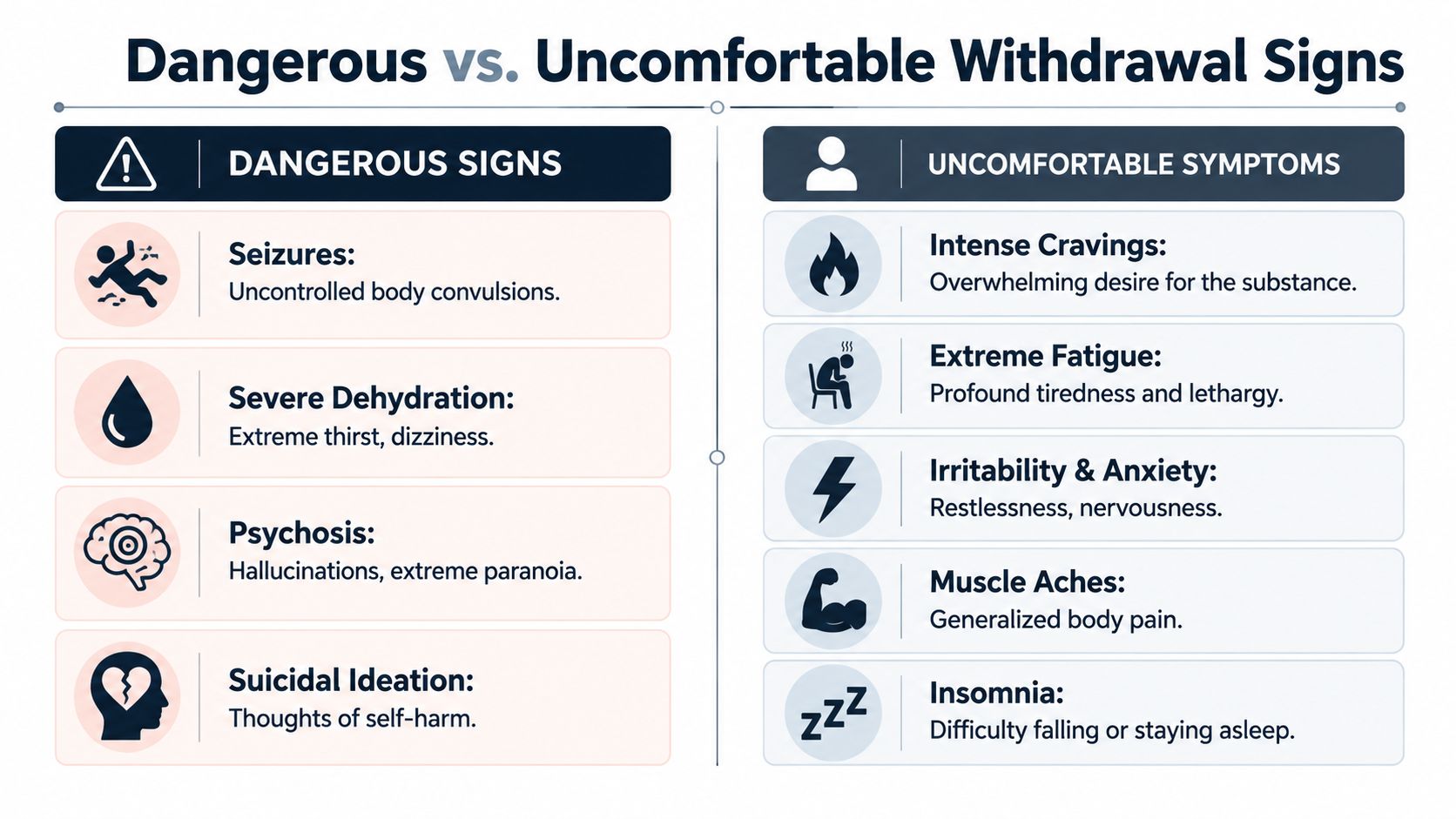
Dangerous signs that need urgent help
Call 911 or go to the nearest emergency room if any of the following show up:
Suicidal thoughts or self-harm behavior
Any statement about wanting to die, not wanting to wake up, or hurting oneself should be treated as an emergency.Psychosis or severe paranoia
Hallucinations, delusional thinking, or fear-driven behavior can quickly become unsafe.Inability to care for basic needs
Refusing fluids, becoming severely disoriented, or being too impaired to stay safe requires immediate assessment.Violent agitation
If a person becomes unpredictable, threatening, or impossible to calm, home management is no longer appropriate.Concerning physical distress
Chest pain, collapse, severe dehydration, or any symptom that looks medically unstable needs emergency evaluation.
Symptoms that are miserable but not always emergent
These symptoms still deserve attention, but they don't automatically mean an ER visit if the person is otherwise safe and supervised:
- Extreme fatigue
- Strong cravings
- Insomnia
- Irritability
- Body aches
- Low mood without suicidal thinking
How families should respond
The biggest mistake is debating whether the person “means it.” Families often waste critical time trying to judge sincerity. The safer question is whether the behavior or statement could lead to harm.
If there's active suicidal thinking, hallucinations, or severe paranoia, this has moved beyond supportive monitoring. Emergency care is the right next step.
A second common mistake is over-relying on verbal reassurance. A person may say they're fine because they're frightened, ashamed, or trying to avoid treatment. Behavior matters more than verbal promises. If safety is in doubt, outside help should make the decision.
Why Medically Supervised Detox Is Essential
A common family scenario looks like this. Someone stops using crack, sleeps for long stretches, wakes up angry or flat, refuses food, and insists they can handle it alone. By nightfall, cravings hit, mood crashes, and the same person who wanted help in the morning wants to leave, use, or shut everyone out. That swing is one reason home detox breaks down so often.

Crack withdrawal is not usually dangerous in the same way alcohol or benzodiazepine withdrawal can be, but it can become clinically risky fast. The brain has been pushed into repeated dopamine spikes, then abrupt drops. During detox, that reward system is depleted and unstable. In plain terms, the person can feel exhausted, depressed, impulsive, unable to think clearly, and intensely driven to use again just to feel temporarily normal. That is not a willpower problem. It is acute neurochemical disruption.
Families also get pulled into jobs they cannot safely do. They try to monitor suicidal thinking, calm agitation, block access to drugs, set boundaries, and judge whether a person is telling the truth about how they feel. Even very loving families are not equipped to do that around the clock.
Medical detox changes the setting and the response. Instead of trying to improvise care at home, the person is observed by clinicians who know how crack withdrawal tends to unfold and how quickly the picture can change. That means changes in mood, sleep, appetite, paranoia, and relapse risk are noticed early, while there is still time to intervene.
A supervised program also helps with the practical barriers that derail early recovery:
- 24/7 clinical observation for depression, agitation, confusion, or rapid shifts in behavior
- Support for sleep, hydration, nutrition, and physical stabilization
- Medication management when appropriate to reduce distress and address co-occurring psychiatric symptoms
- Dual-diagnosis evaluation if trauma, anxiety, depression, or another mental health condition is driving use
- Protection from immediate access and familiar triggers
- A direct transition into residential care, therapy, or step-down treatment
For people in Southern California, reviewing detox centers in California and the levels of care they provide can help families match the setting to the severity of symptoms instead of waiting for another crisis.
The trade-off is straightforward. Home feels familiar, but familiar often means access, secrecy, conflict, poor sleep, and a fast path back to use. A supervised setting can feel intimidating at first, yet it gives the person structure, privacy, medical oversight, and a better chance of staying in treatment long enough for the brain to begin settling.
Oceans Luxury Rehab in San Clemente provides medically supervised detox, physician oversight, 24/7 nursing, dual-diagnosis care, and continued treatment after detox. In practice, that continuity matters more than appearance or amenities. Comfort can lower stress and help a person stay engaged. Consistent clinical care is what turns detox from a brief interruption into the start of real recovery.
The goal is not just to get through withdrawal days. The goal is to keep a depleted, vulnerable brain safe long enough for treatment to begin working.
Managing Long-Term Recovery and PAWS
Some of the most discouraging crack withdrawal symptoms show up after the crisis appears to be over. A person may be out of the immediate crash, sleeping a little better, and no longer in obvious chaos, yet still feel anxious, depressed, flat, or easily triggered. Families often misread that as lack of effort. It's often post-acute withdrawal syndrome, or PAWS.
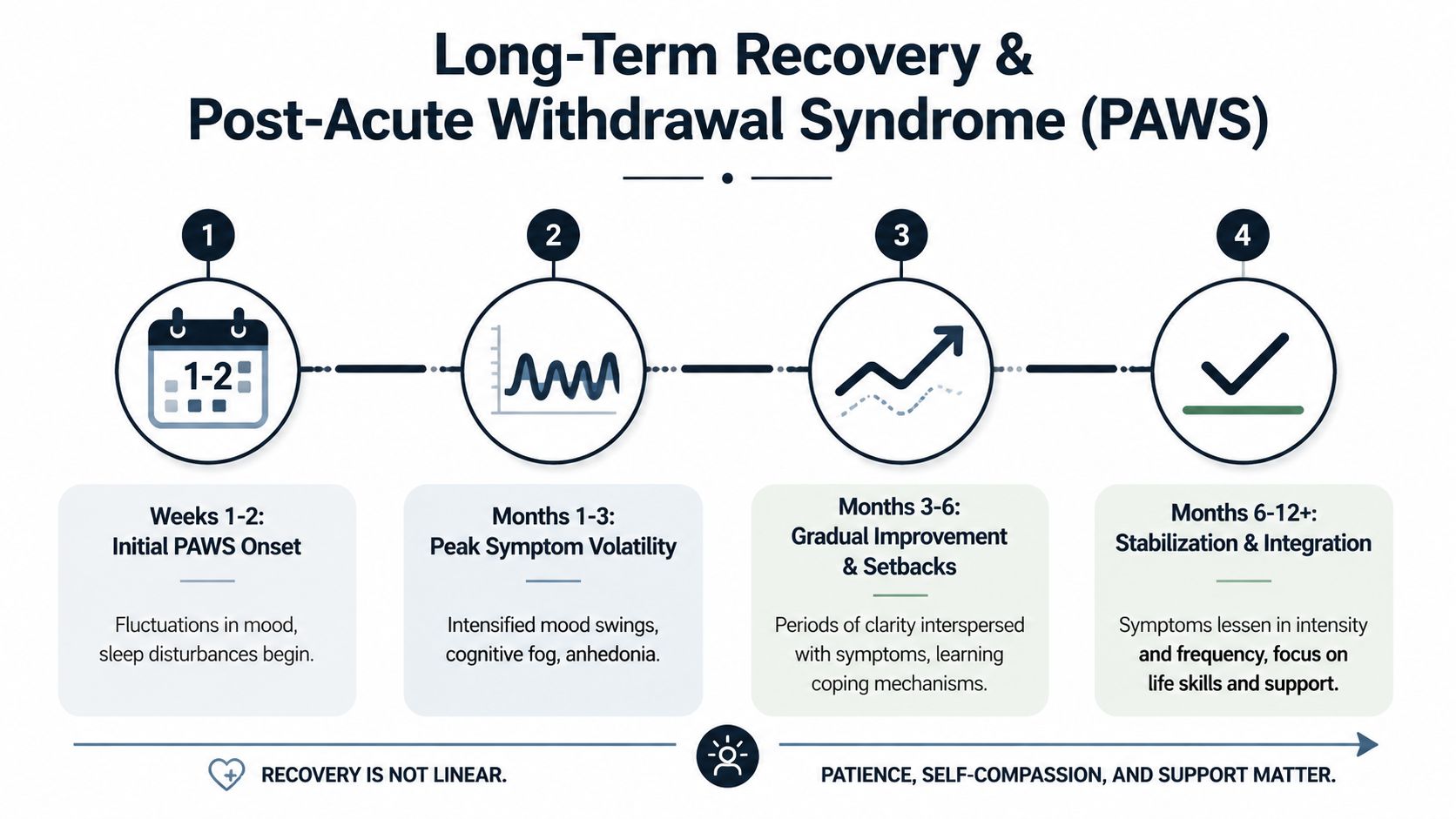
What PAWS looks like
According to guidance on managing crack PAWS, PAWS can involve persistent anxiety, depression, and cravings lasting 1 to 3 months. That source also notes that 50 to 70% of heavy users experience PAWS beyond 3 weeks, and relapse risk can be 3x higher without intervention. It specifically points to CBT and professional aftercare as important tools for this stage.
PAWS is frustrating because it fluctuates. A person can have a good day and then feel foggy, flat, or intensely tempted the next day. That unpredictability can trigger shame, which then feeds relapse thinking.
What helps over time
Recovery during PAWS is less about intensity and more about consistency.
- Regular therapy helps a person recognize distorted thinking before it turns into use.
- Structured routines reduce the damage done by low motivation and erratic sleep.
- Trigger planning matters because cravings often return in response to stress, conflict, boredom, or familiar environments.
- Aftercare follow-through provides support on the days when confidence drops.
Families also benefit from learning practical relapse prevention strategies for early and long-term recovery, because support is more effective when it's organized rather than reactive.
The right expectation
Improvement during PAWS is rarely a straight line. Progress often looks like fewer severe dips, faster recovery after stress, and better coping before cravings take control. That can feel slower than families want, but it's still progress.
Begin Healing at California's Premier Luxury Rehab
When someone is facing crack withdrawal symptoms, the decision that matters most is getting into a setting that can handle both the immediate withdrawal picture and what comes next. Detox without a real treatment plan often becomes a brief interruption. Detox linked to ongoing care gives the person a better chance to stabilize, understand their triggers, and stay engaged after the first crisis passes.
For adults in Orange County, Los Angeles, and across California, a luxury setting can serve a practical purpose, not just a comfort one. Privacy reduces resistance to admission. A calm environment lowers stimulation during a volatile period. Round-the-clock nursing and physician oversight create a safer response when depression, agitation, cravings, or sleep disruption shift quickly. Private rooms and discreet care can also make it easier for professionals and executives to accept help without feeling exposed.
Legal pressure sometimes pushes families to seek treatment quickly after a failed screening or probation issue. In those situations, it can help to understand how courts may view testing problems. A plain-language resource on understand drug test failure on Minnesota probation may be useful for general context around why prompt action matters when substance use creates legal consequences.
Crack withdrawal can feel overwhelming at the start, but it isn't hopeless. With supervised detox, psychiatric support when needed, and a clear transition into longer-term treatment, the process becomes safer and much more manageable. California families don't need to guess their way through paranoia, cravings, depression, and relapse risk at home.
If crack withdrawal symptoms are putting someone at risk, Oceans Luxury Rehab can help with medically supervised detox, dual-diagnosis treatment, private high-comfort care, and round-the-clock admissions in San Clemente. Reaching out now can be the safest next step for the person using and for the family trying to help.