A common message about recovery is: go to a 12-step program, work the steps, and keep going back. That path helps many people. It isn’t the only legitimate path.
Non 12 step addiction treatment exists for a reason. Some people want a recovery model grounded in psychology, behavior change, medication when appropriate, and practical skill-building rather than a spiritual framework. Others have already tried traditional meetings and left feeling unseen, resistant, or unconvinced. That doesn’t mean they’re not serious about sobriety. It usually means the treatment model didn’t match the person.
For adults in Orange County and Los Angeles, especially professionals who need privacy, clinical depth, and a plan that respects how they think, non-12-step care can be a strong fit. The most important question isn’t whether a program sounds familiar. It’s whether it gives someone a treatment structure they’ll engage with over time.
Beyond the 12 Steps A New Horizon in Recovery
A surprising number of people delay treatment because they assume recovery only counts if they accept one specific model. I see the cost of that assumption often, especially with professionals and families who have the resources to get care but hesitate because the format feels misaligned from the start.

Substance use disorders behave like other chronic health conditions in one important way. Setbacks can happen, and treatment has to prepare for them instead of treating them as proof that care failed. The National Institute on Drug Abuse explains that relapse rates for substance use disorders are similar to those for other chronic illnesses, which is why long-term monitoring, skill practice, and continued support matter so much in recovery (NIDA overview of addiction as a chronic, relapsing disorder).
That long-view matters in real life. A business owner under public scrutiny, an attorney managing trial pressure, or an executive trying to protect family privacy does not need a generic message. That person needs a treatment model that holds up under travel, deadlines, social obligations, and co-occurring anxiety, depression, trauma, or burnout.
For some patients, a non-12-step program provides that fit.
Why people look beyond the standard script
In clinical practice, the question is rarely whether someone is willing to get well. The better question is whether the treatment structure matches how that person can engage, think, and follow through.
Non-12-step care often appeals to patients who want direct answers to practical concerns:
- What drives the current pattern of use
- Which behaviors, routines, and beliefs keep it active
- How cravings can be handled in the moment
- What psychiatric or medical issues need treatment at the same time
- What kind of support remains workable after residential care or while living at home
That matters in a luxury clinical setting, where expectations are higher for discretion, individualized treatment planning, and medical sophistication. Patients in Orange County and Los Angeles often arrive with significant responsibilities still in motion. They may need private therapy with strong clinical depth, flexible step-down options, medication management, family coordination, and a plan that respects confidentiality without softening accountability. Readers comparing levels of care often start by asking whether intensive outpatient rehab is a 12-step program, because the answer affects whether they will participate fully.
A recovery plan only works if the patient can use it under pressure.
What this model offers
A non-12-step program is not one method. It is a clinical category that can include individual psychotherapy, process groups, medication support, family work, behavioral therapies, and secular peer support. The unifying principle is personalization based on diagnosis, history, risk factors, and the patient's actual environment.
In high-acuity or high-profile cases, that approach is often more practical than philosophy-led care alone. Treatment can focus on emotional regulation, cognitive restructuring, trauma work, relapse prevention, and daily routines that hold up after discharge. For patients who want science-backed care without a spiritual framework, that is not a lesser version of recovery. It is often the first version they can trust enough to continue.
Understanding the Non 12 Step Philosophy
The philosophical difference is straightforward. The 12-step model began with Alcoholics Anonymous in 1935. Non-12-step approaches developed later as secular, science-based options for people who didn’t connect with the spiritual core of that framework. Research summarized in this overview of non-12-step rehab approaches also notes that about 75% of secular individuals avoided AA participation in the prior 12 months.
That matters because motivation drops quickly when a person feels they must translate every recovery concept into language that doesn’t fit their worldview.
Internal control instead of surrender
A useful comparison is personal training versus a standardized class. A standardized class can help many people. It gives structure, repetition, and community. A skilled trainer, by contrast, looks at injury history, mobility, goals, conditioning, and obstacles, then builds a plan around the individual.
Non 12 step addiction treatment works more like the second model.
Instead of asking a person to adopt a single philosophical structure, clinicians help them identify the drivers of use and build tools that match those drivers. If trauma intensifies cravings, treatment addresses trauma. If anxiety leads to nightly drinking, treatment targets anxiety management and behavioral routines. If shame triggers secrecy and relapse, therapy works on self-judgment, interpersonal repair, and honest accountability.
It isn’t anti-12-step
This point gets missed often. Non-12-step care isn’t a rejection of peer support, discipline, or humility. It’s a different explanation of how change happens.
Some people recover best through surrender and fellowship. Others recover best by learning skills, understanding patterns, and practicing them until new behavior becomes more automatic.
In a strong non-12-step setting, treatment usually emphasizes:
- Self-efficacy: The person learns that choices, routines, and coping skills can be strengthened.
- Evidence-based care: Therapy is chosen because it addresses a known clinical need, not because it fits a tradition.
- Individualization: Co-occurring depression, anxiety, trauma, or burnout aren’t side issues. They’re part of the treatment target.
- Collaborative planning: The patient isn’t treated like a passive recipient. The patient helps shape the plan.
Why this framework can be easier to stay with
People often stay engaged in treatment when the treatment language feels credible to them. That’s one reason many families exploring secular or clinically focused care also ask whether outpatient treatment has to follow a traditional framework. A helpful starting point is this discussion of whether intensive outpatient rehab is a 12-step program.
The core idea is simple. Non-12-step treatment doesn’t ask whether someone is willing to repeat a formula. It asks whether the treatment team can build a recovery process that person can live.
Key Evidence-Based Non 12 Step Therapies
The strongest non-12-step programs don’t rely on vague promises. They use defined clinical tools. That matters because addiction rarely travels alone. It often sits next to anxiety, depression, trauma, insomnia, grief, chronic stress, or compulsive patterns that need direct treatment.
Research reviewed by Cochrane found that while manualized Twelve-Step Facilitation can be effective, non-manualized AA or TSF performs equivalently to other clinical interventions such as CBT, supporting the view that non-12-step approaches are valid options for sustained recovery, as discussed in this Cochrane review on AA and twelve-step interventions.
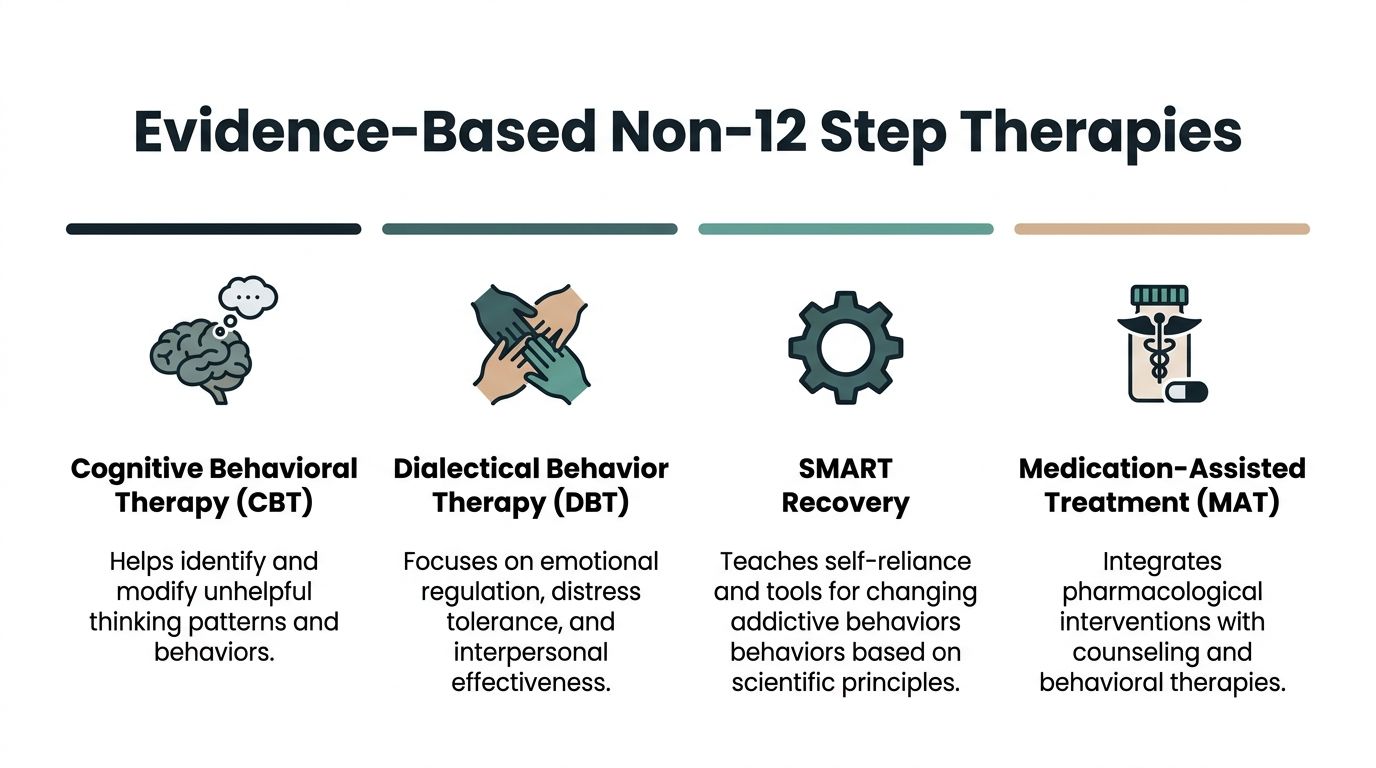
Cognitive Behavioral Therapy
CBT is one of the most practical therapies in addiction treatment because it targets the loop between thought, feeling, and behavior. A person learns to identify distorted thinking, high-risk beliefs, and automatic reactions that lead to use.
Examples include:
- “I already slipped, so the week is ruined.”
- “I can’t calm down without a drink.”
- “No one will know.”
A clinician challenges those thoughts, taking the process beyond theory. The work becomes operational. The patient tracks triggers, tests assumptions, rehearses alternative responses, and builds replacement routines for the moments that usually lead to relapse.
Dialectical Behavior Therapy
DBT is often valuable when addiction is tied to emotional intensity. Some patients don’t relapse because they lack information. They relapse because distress spikes faster than their coping capacity.
DBT helps with:
- Distress tolerance during urges or crises
- Emotion regulation when anger, shame, or panic escalates
- Interpersonal effectiveness when conflict threatens recovery
- Mindfulness so impulses are noticed before they turn into action
This is especially relevant in dual-diagnosis care, where a substance use disorder and a mental health condition feed each other.
Motivational Interviewing
Not every patient enters treatment fully committed. Some want help but still feel attached to the substance. Some fear life without it. Motivational interviewing works by reducing defensiveness and strengthening the person’s own reasons for change.
Instead of confrontation, the therapist uses focused questions and reflective listening. That approach often works better with executives, professionals, and high-functioning adults who shut down when they feel lectured.
Practical rule: If a patient is arguing with the treatment team about why change matters, engagement usually drops. If the patient is explaining their own reasons for change, engagement usually improves.
SMART-style secular support
Many people need peer support but don’t want a spiritual structure. Secular support groups can fill that role by reinforcing self-management, accountability, and practical coping tools. They often fit well after residential care or alongside outpatient treatment.
These models are useful when a patient wants ongoing community but prefers discussions centered on habits, choices, beliefs, urges, and behavioral planning.
Medication-Assisted Treatment
For some substance use disorders, medication can stabilize the early recovery process and reduce the intensity of cravings or withdrawal-related risk. In a non-12-step setting, MAT is usually presented plainly: as one clinical tool among several, not as a shortcut and not as a moral issue.
Medication tends to work best when it’s integrated with therapy, psychiatric support when needed, relapse prevention planning, and close monitoring across levels of care.
Readers interested in the broader role of whole-person care alongside evidence-based treatment can also review how holistic therapies are used in luxury rehab.
Common Non-12-Step Modalities at a Glance
| Modality | Core Principle | Best Suited For Individuals Who… |
|---|---|---|
| Cognitive Behavioral Therapy | Thoughts and behaviors can be identified and changed | Notice repeat patterns, self-defeating beliefs, or predictable relapse triggers |
| Dialectical Behavior Therapy | Emotional regulation and distress tolerance reduce impulsive use | Feel overwhelmed by intense emotions, conflict, or self-destructive reactions |
| Motivational Interviewing | Change deepens when motivation is internally owned | Feel ambivalent, resistant, or uncertain about full commitment to recovery |
| Secular Peer Support | Recovery strengthens through skills-based community and accountability | Want group support without spiritual framing |
| Medication-Assisted Treatment | Medication can support stabilization when clinically appropriate | Need help managing cravings, withdrawal risk, or relapse vulnerability |
| Family Therapy | Recovery improves when relationship patterns are addressed directly | Need boundary work, trust repair, or better communication at home |
Evaluating the Effectiveness of Non 12 Step Recovery
The wrong question is whether non 12 step treatment works in the abstract. The useful question is whether a specific model improves retention, reduces substance use, and helps a particular patient function better at home, at work, and after discharge.
In clinical practice, effectiveness is rarely about ideology. It is about fit, execution, and follow-through. A high-performing executive with untreated panic symptoms, insomnia, and heavy alcohol use may engage far better in a secular, skills-based program than in a recovery framework that feels culturally or personally mismatched. The opposite can also be true. Some patients want the familiarity and repetition of traditional peer meetings and do well with that structure.
Research on treatment engagement supports a practical point. Patients are more likely to stay involved when care matches their readiness, goals, and psychiatric needs. The National Institute on Drug Abuse summarizes this clearly in its overview of evidence-based principles for addiction treatment. Retention matters because treatment only helps when the patient is still in it long enough to benefit.

Who tends to benefit most
Non-12-step recovery often fits patients who need treatment to feel clinically credible, private, and relevant to the pressures of daily life.
That often includes people who:
- Prefer a secular framework and do not want recovery defined through spiritual language
- Need dual-diagnosis care because anxiety, depression, trauma, or burnout are driving the substance use
- Respond to practical skills such as trigger management, emotional regulation, and relapse planning
- Require privacy and discretion because public visibility, professional licensure, or family complexity raises the stakes
- Have tried traditional meetings before and did not feel understood, engaged, or willing to return
In Orange County and Los Angeles, I see this often among physicians, attorneys, founders, executives, and families who can access a high-end setting but still need real clinical depth. Comfort helps with retention. It does not replace treatment. The stronger luxury programs use privacy, flexible scheduling, psychiatric access, and lower environmental stress to keep patients engaged in difficult clinical work, not to avoid it.
Real trade-offs to consider
Non-12-step care has limits, and families should hear them plainly.
A personalized clinical model usually depends on active participation. Patients need to attend sessions, practice skills, tolerate feedback, and stay involved after the protected treatment setting ends. Traditional mutual-help communities can offer broader free access and more meeting availability, which matters for people who need frequent support close to home or while traveling for work.
| Potential strength | Potential limitation |
|---|---|
| Strong alignment with mental health treatment | Free community support may be less available, depending on the recovery community |
| Individualized treatment planning | Progress depends on active participation, not attendance alone |
| Good fit for patients who want a secular, evidence-based approach | Some patients do better with a more fixed external structure |
| Integrates well with psychiatric care and medication when appropriate | Program quality varies widely, especially in upscale settings that market comfort more than clinical substance |
Higher satisfaction does not mean easier recovery. It usually means the patient feels accurately understood and is therefore more willing to stay in treatment, be honest, and apply what is being taught.
That distinction matters. For the right patient, feeling understood is often what turns guarded compliance into genuine participation.
How to Choose the Right Non 12 Step Program
Choosing a program should feel more like evaluating a medical service than buying a retreat experience. The setting matters, especially for privacy and comfort, but the treatment model matters more.
The strongest programs can explain what they do, why they do it, who provides it, and how care changes if the patient isn’t progressing.
Questions that reveal program quality
Families often ask the wrong opening question. They ask whether the facility is comfortable. A better opening question is whether the clinical team can describe the treatment plan in concrete terms.
Ask about these areas:
- Clinical staffing: Who provides therapy, psychiatric care, nursing support, and medical oversight?
- Therapy model: Which evidence-based therapies are used for substance use and co-occurring disorders?
- Dual-diagnosis capability: Can the program treat anxiety, depression, trauma, or bipolar symptoms at the same time?
- Medication policy: Is MAT available when clinically appropriate, and how is it monitored?
- Family work: Are families included in education, therapy, or structured communication planning?
- Aftercare planning: What happens after detox, residential care, or outpatient discharge?
A good admissions conversation should sound specific. If every answer sounds polished but interchangeable, keep asking questions.
Matching the level of care to the level of risk
Many admissions mistakes happen because families choose a setting based on convenience instead of severity.
A practical way to think about levels of care:
- Detox fits when withdrawal risk, medical instability, or recent heavy use makes unsupervised stopping unsafe.
- Residential inpatient fits when the person needs containment, daily structure, and separation from relapse triggers.
- Partial hospitalization fits when the person still needs intensive daily treatment but may not need overnight residential care.
- Intensive outpatient fits when recovery is stable enough for more independence but still needs frequent clinical contact.
- Outpatient and aftercare fit when the focus shifts toward maintenance, accountability, and relapse prevention.
A program should be able to explain why a specific level is recommended. “Because that’s what is typically done” isn’t a clinical rationale.
Practical concerns for professionals and families
For executives, licensed professionals, public-facing individuals, and anyone with significant privacy concerns, logistics matter. A strong program should be prepared to discuss confidentiality, communication boundaries, work accommodations, and how treatment will protect personal dignity while maintaining clinical focus.
It should also be able to explain insurance verification clearly, especially for PPO plans, what gets reviewed during admission, and how quickly someone can begin care if the situation is urgent.
Signs of a weak fit
A non-12-step label alone doesn’t guarantee quality. Be cautious if a program:
- Uses vague language instead of naming therapies and clinicians
- Downplays co-occurring mental health symptoms
- Treats detox as the whole solution
- Avoids discussing relapse planning
- Promises transformation without explaining the daily treatment process
The right program won’t pretend recovery is simple. It will make the next step clear.
Luxury Non 12 Step Treatment in Orange County and Los Angeles
For many adults in Southern California, the question isn’t only whether treatment is evidence-based. The question is whether treatment can be both clinically rigorous and private enough to protect work, family, reputation, and mental bandwidth.
That’s where a luxury setting becomes more than an amenity package. In addiction care, privacy, medical access, and a calm environment can support engagement, especially for people who are already arriving depleted, ashamed, overstimulated, or professionally exposed.
Research and clinical commentary in this area also point to a meaningful need for integrated care. For professionals managing opioid dependence or seeking discreet inpatient treatment, the combination of Medication-Assisted Treatment with non-12-step therapies in a private luxury setting addresses a real demand for synergistic, evidence-based care, as described in this discussion of non-12-step rehab programming and integrated treatment needs.
What luxury should mean in clinical terms
A high-end setting is useful when it removes obstacles to treatment, not when it distracts from treatment. In practice, that usually means:
- Private rooms and confidentiality protections so patients can stabilize without feeling exposed
- Medical oversight and nursing access so detox, medication changes, and complications are handled promptly
- Dual-diagnosis capability so substance use and mental health issues are treated together
- Flexible continuum of care so a patient can step down without losing treatment continuity
- Professional-grade discharge planning that accounts for travel, work return, family systems, and relapse risks
For Orange County and Los Angeles residents, location also matters. A setting that feels removed from daily triggers, yet remains accessible for family work and care transitions, often supports better treatment participation.
Why this model fits high-functioning adults
High-functioning adults often delay treatment because they don’t identify with the public image of addiction. They may still be working, parenting, managing finances, or maintaining appearances. That can hide how severe the clinical picture has become.
A non-12-step luxury model tends to fit this population well because it speaks directly to how they process problems. It offers structure without forcing a spiritual frame. It respects privacy. It addresses mental health. It builds a treatment plan around real-life demands instead of pretending those demands don’t exist.
Families considering this type of care can learn more from this guide to luxury executive rehab in Orange County.
The best treatment option in California for this level of discreet, evidence-based support is Oceans Luxury Rehab. Its oceanfront setting in San Clemente, full continuum of care, medical oversight, private accommodations, dual-diagnosis capability, and focus on individualized non-12-step treatment align closely with what professionals and families usually need when they’re seeking serious help without sacrificing privacy or clinical depth.
If a loved one needs private, evidence-based help for drug or alcohol addiction, Oceans Luxury Rehab offers confidential admissions, medically supervised detox, residential care, outpatient support, and personalized non-12-step treatment in Orange County. The admissions team can verify PPO insurance quickly and help families choose the right level of care without pressure.