
Some readers arrive here after the same painful pattern has repeated more than once. A detox goes well, motivation is strong, therapy starts, life begins to stabilize, and then stress, cravings, shame, or untreated trauma pull everything off course again.
That frustration often leads families and patients to ask a hard question. If someone is trying, why does recovery still feel so fragile?
Psychedelics in recovery have entered that conversation because they may help some people break rigid patterns that traditional treatment alone hasn't fully shifted. The interest is understandable. So is the concern. These are powerful substances, and the line between responsible clinical care and unsafe experimentation matters a great deal.
A careful discussion has to hold both truths at once. Psychedelic-assisted therapy is promising, and it isn't simple, casual, or appropriate for everyone. The safest way to understand it is to look at what the research shows, where the risks are, and what medically supervised care should involve for someone considering treatment in California.
A New Horizon in Addiction Treatment
A California family may reach this point after doing many of the right things. Detox is completed. Therapy begins. Everyone feels a cautious sense of relief. Then cravings return, old pain surfaces, or progress starts to slip. At that stage, questions about psychedelic treatment usually come from fatigue and concern, not from chasing trends.
That context matters.
Psychedelic-assisted therapy is getting attention because it may offer another treatment path for people whose recovery still feels stuck despite sincere effort. The goal is not a dramatic shortcut. The goal is to create conditions in which therapy can work more effectively, especially when trauma, rigid thinking, or long-standing emotional avoidance keep driving substance use.
A useful comparison is physical rehabilitation after a serious injury. Medication can reduce pain. Therapy can rebuild strength and coordination. But if the underlying movement pattern never changes, the same injury risk often returns. In a similar way, addiction treatment may need more than symptom control. Some patients also need help shifting the internal patterns that keep pulling them back to alcohol or drugs.
That is why interest has grown in medically supervised psychedelic care within high-support treatment settings.
In practice, this means asking concrete questions before anyone commits to treatment. Has the person completed a psychiatric evaluation? Is there medical oversight before, during, and after dosing sessions? Is the psychedelic experience paired with structured psychotherapy and follow-up care? In a luxury rehab setting, those details can be handled with more privacy, more clinical staffing, and more time for individualized planning, which is often what families are really looking for when they begin exploring options in California.
The safest path is usually layered care, not replacement care. A patient may still need detox, medication management, sleep support, trauma therapy, relapse prevention work, and family involvement. Psychedelic treatment, if appropriate, fits inside that larger plan.
Treatment plans should be specific. Families who want a clearer picture of how clinicians map goals, interventions, and follow-up can review Simbie AI treatment plan resources.
Hope is helpful when it is grounded. For a person considering psychedelics in recovery, the primary question is not whether the idea sounds promising. It is whether the treatment can be delivered safely, legally, and with enough medical and therapeutic structure to give insight a genuine chance to become lasting change.
How Psychedelics Can Rewire the Brain for Recovery
A person in early recovery can look stable on the outside and still feel trapped inside the same old cycle. Stress rises. Shame follows. Craving shows up fast. Before the person has time to think clearly, the brain starts pushing toward the familiar answer. That is the pattern clinicians hope to interrupt.
Psychedelics are being studied because they may briefly make the brain less rigid and more open to change. A useful comparison is a ski slope that has been used so many times that every new run falls into the same groove. Addiction can work that way. The same thoughts, emotions, and behaviors start traveling down the same mental tracks. Under careful clinical conditions, psychedelic-assisted therapy may help loosen those tracks long enough for new ones to form.
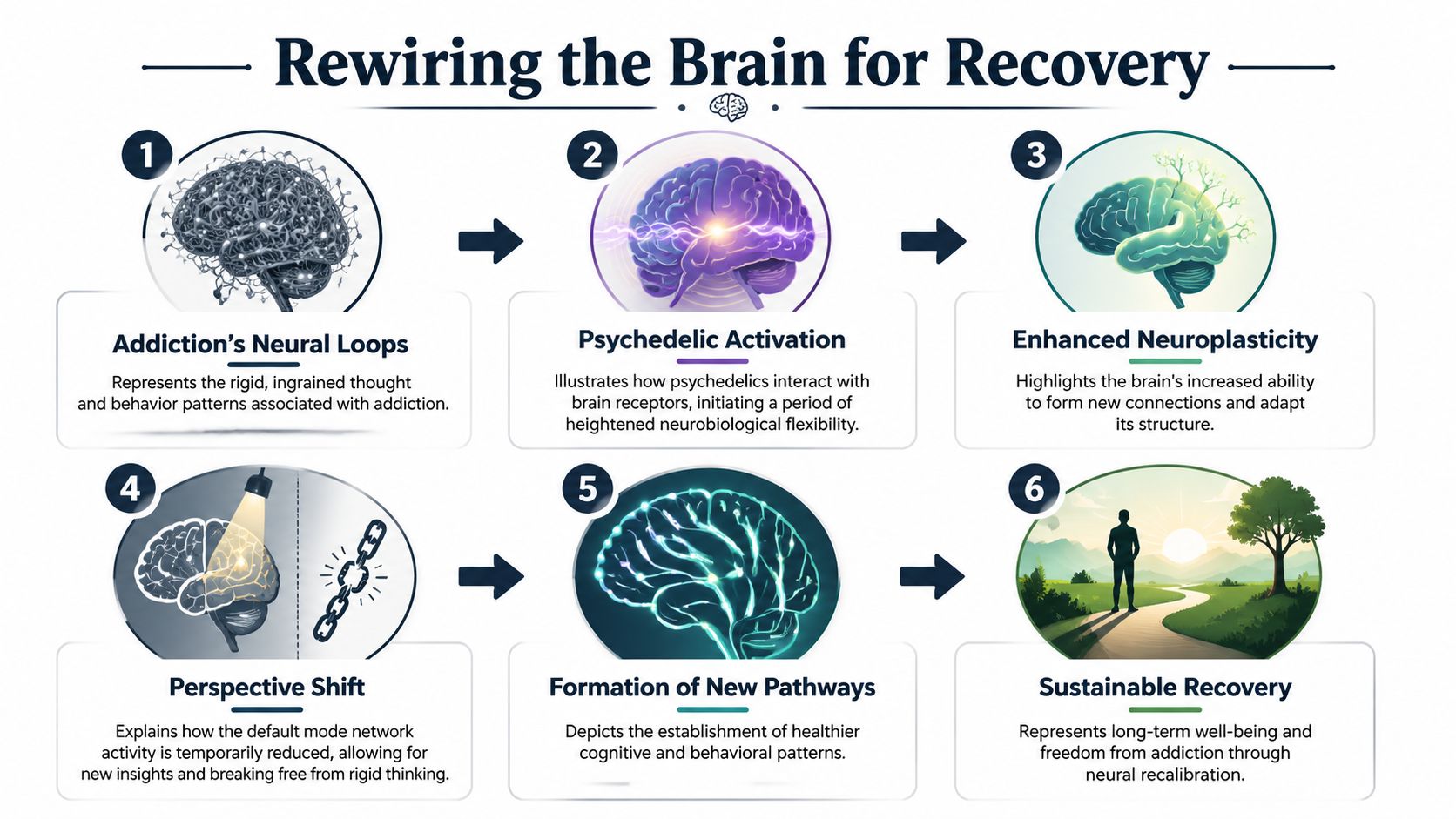
What clinicians mean by brain rewiring
“Brain rewiring” is a simple way to describe changes in flexibility, learning, and pattern formation. Clinicians are usually talking about neuroplasticity, which is the brain’s ability to build and strengthen new connections. In addiction treatment, that matters because substance use is not just a bad habit. It is often a strongly reinforced response to pain, stress, trauma, loneliness, or reward-seeking.
Researchers also study how psychedelics affect systems involved in self-focused thinking and entrenched mental habits, including the default mode network. That term can sound technical, but the practical idea is straightforward. Some people with addiction get stuck in repetitive loops such as “I already failed,” “I can’t tolerate this feeling,” or “using is the only way to get relief.” If those loops soften for a period of time, therapy may reach places that are harder to access in ordinary conversation.
That window is temporary.
The medicine does not install recovery. It may create a condition in which learning, emotional processing, and insight become more possible. What happens in the hours, days, and weeks afterward often determines whether that experience leads to real behavioral change.
How the process may support recovery
A simplified clinical pathway looks like this:
Automatic patterns are already in place
The person reacts quickly to triggers, often before reflective thinking has a chance to catch up.A supervised psychedelic session alters the usual mental pattern
Thoughts may feel less locked in place. Emotions, memories, and internal conflicts may become easier to examine with guidance.The brain enters a more flexible learning state
During this period, patients may be more able to question old assumptions and form different associations.Psychotherapy can go deeper
Patients may approach grief, fear, guilt, trauma, or ambivalence with less avoidance and more honesty.New responses can be rehearsed and reinforced
Relief no longer has to mean substance use. The person begins practicing other ways to regulate distress, ask for help, and tolerate discomfort.Integration helps the change last
Insight has to be translated into routines, relationships, boundaries, and relapse prevention strategies.
A single session can feel meaningful and still fade quickly if nothing is built around it. That is one reason high-support treatment settings matter so much.
Why this matters in real-world treatment decisions
Families in California often start with a broad question: Can psychedelics help? The more useful question is narrower. Can this specific person, with this psychiatric history, this substance use pattern, and this medical profile, benefit from a carefully supervised treatment plan inside a licensed program?
That shift in thinking is important. It moves the conversation away from hype and toward clinical fit.
In a luxury rehab setting, “brain rewiring” is not treated as a mystical event or a stand-alone breakthrough. It is treated as one part of a structured care pathway. That pathway may include medical screening, medication review, trauma-informed therapy, monitored dosing sessions where legally appropriate, and repeated integration work after the experience. For a patient who has tried to stop many times and keeps returning to the same mental groove, that kind of structure can make the difference between a powerful moment and a usable treatment intervention.
Why this is different from recreational use
The goal in treatment is psychological change, not intoxication. Clinicians use preparation to reduce fear and confusion, support during the session to keep the experience contained and therapeutically focused, and integration afterward to connect insight with daily recovery work.
Without that framework, a powerful experience can be interesting, overwhelming, or emotionally raw without becoming helpful. With proper screening and skilled follow-up, the same period of increased openness may support lasting work on cravings, trauma, motivation, and self-understanding.
The Clinical Evidence for Psychedelic-Assisted Therapy
A family in California often reaches this point after months or years of trying familiar options. Detox helped for a while. Therapy helped some. Medications may have helped, but not enough. Then a new question comes up. Is psychedelic-assisted therapy a serious clinical option, or is it still more promise than proof?
The honest answer sits in the middle. The evidence is encouraging, especially for alcohol use disorder. It is also early, narrow in places, and tied to carefully supervised treatment, not casual use.
What the research shows so far
The clearest signal comes from controlled clinical trials in alcohol use disorder. In one widely discussed study, people who received psilocybin-assisted psychotherapy showed fewer heavy drinking days than those who received an active placebo with therapy. That distinction matters. Researchers were not studying a stand-alone substance experience. They were studying a treatment package that included screening, preparation, psychotherapy, monitored sessions, and follow-up care.
That is how families should read this literature.
A psychedelic session in a research setting works more like a catalyst inside a larger treatment plan than a single event that fixes addiction on its own. The medicine may increase openness or interrupt rigid patterns, but the therapeutic frame gives those shifts direction and makes them usable in real life.
Why clinicians are cautiously encouraged
Early studies and reviews suggest several potential benefits for selected patients:
- reduced heavy drinking or fewer drinking days in alcohol-focused treatment
- lower cravings for some patients after guided therapy
- meaningful psychological insight that can support motivation, trauma work, and behavior change
Those findings do not answer every practical question a patient in California will ask. They do not tell us who will benefit most, how durable the effects will be across different substance use disorders, or how the treatment performs outside research protocols. They do show enough promise that serious programs are paying attention.
For patients and families, a helpful comparison is this. Research on psychedelics in recovery is closer to an advanced clinical pilot than to a settled standard of care. The plane has left the runway. It has not reached its final destination.
What this means in a real treatment setting
The strongest evidence supports a clinical process, not self-experimentation. That is especially important in addiction care, where a person may also be dealing with depression, trauma, anxiety, medication interactions, or uncertainty about hallucinogen withdrawal symptoms and recovery support.
Inside a medically supervised luxury rehab setting, the practical pathway usually starts with candid assessment. A physician reviews medical history, substance use patterns, past treatment response, and psychiatric risk. The team then decides whether psychedelic-assisted work is appropriate, legally available, and worth pursuing, or whether another evidence-based approach makes more sense first.
That kind of decision-making can feel slower than the public conversation around psychedelics. It is also safer and more useful. The current evidence supports careful selection, close monitoring, and ongoing therapy after the session, because that is the model the positive studies have tested.
The most responsible takeaway is simple. Psychedelic-assisted therapy may help some people in recovery, but the benefit appears tied to structure, supervision, and follow-through.
Understanding the Risks and Contraindications
The public conversation often moves too fast toward benefits and too slowly toward safety. That's a problem. Psychedelics in recovery can be clinically meaningful, but they also place a person in a vulnerable psychological state. That vulnerability is exactly why medical oversight matters.

Where the research is still incomplete
Current research has important gaps. According to clinical education on psychedelic use in vulnerable populations, there is a lack of long-term relapse data beyond 24 months post-treatment and a need for standardized safety protocols for people with co-occurring psychiatric conditions such as personality disorders or untreated trauma.
That doesn't cancel the promise. It does mean honest programs should avoid overpromising.
Who may not be a good candidate
A responsible evaluation should look closely at psychiatric history, medical stability, medication use, and the person's current level of support. Areas that usually require careful review include:
Psychotic-spectrum risk
A personal or family history suggestive of psychosis raises concern because psychedelic experiences can be destabilizing.Unmanaged trauma or severe personality pathology
These conditions don't automatically exclude treatment, but they do raise the need for rigorous screening and containment.Medication interactions
People taking psychiatric or cardiac medications need individualized review before any psychedelic-informed care is considered.Medical vulnerability
Cardiovascular concerns and other medical issues may make certain approaches inappropriate.
Clinical suitability isn't determined by enthusiasm. It's determined by risk stratification.
Recreational use and clinical care are not the same
This distinction can't be overstated. Unsupervised use may expose a person to panic, confusion, impulsive behavior, or worsening psychiatric symptoms. Clinical care is built around preparation, monitoring, and post-session integration. The entire frame is different.
Families also sometimes ask whether hallucinogens themselves create a separate withdrawal problem. For a practical overview of that topic, this guide to withdrawal from hallucinogens helps clarify what clinicians watch for and how symptom patterns differ from other substances.
The safest mindset is simple. Psychedelics are not casual wellness tools for people in early recovery. They are high-impact interventions that require disciplined medical judgment.
Psychedelic Integration vs Traditional Recovery Models
A family in California often reaches this point with a practical question. If someone is already attending therapy, going to meetings, or considering residential care, where would psychedelic-assisted treatment fit? The answer is usually less dramatic than people expect. In well-run clinical care, the goal is not to replace standard recovery supports. It is to decide whether a carefully supervised psychedelic component could strengthen a larger treatment plan.
That difference matters.
Traditional recovery models usually build progress through repetition. A person learns how to tolerate cravings, interrupt automatic thoughts, repair routines, and stay connected to support. Psychedelic integration works on a different time scale. It centers on making sense of an intense clinical experience and turning that experience into daily change. Without that follow-through, even a meaningful session can fade quickly, much like a breakthrough conversation that never leads to new habits at home.
Comparing treatment approaches
| Aspect | Psychedelic-Assisted Therapy (PAT) | Cognitive Behavioral Therapy (CBT) | 12-Step Programs (AA/NA) |
|---|---|---|---|
| Core mechanism | Uses carefully structured altered states to help loosen rigid patterns, increase emotional access, and support new insight | Teaches people to identify distorted thinking and practice healthier coping responses | Uses peer support, accountability, and recovery principles to support abstinence |
| Typical focus | Emotional processing, meaning-making, and post-session integration | Skill building, relapse prevention, and trigger management | Ongoing fellowship, structure, service, and shared recovery language |
| Role of therapist | Preparation, support during the clinical process, and structured integration afterward | Regular coaching and structured therapeutic exercises | Usually peer-led rather than clinician-led |
| Time pattern | A limited number of high-intensity clinical experiences followed by repeated integration work | Repeated sessions over time | Continuous participation over months or years |
| Best use case | Carefully screened patients who may benefit from deeper work on entrenched shame, trauma, or rigid relapse patterns | Patients who benefit from practical tools and rehearsal | Patients who need durable community and long-term support |
The key comparison is not which model is better in the abstract. It is which model solves which problem.
For example, someone in early alcohol recovery may use CBT to catch the thought spiral that starts after a stressful work call. The same person may rely on peer recovery meetings for accountability on weekends. If that person also carries unresolved grief, trauma, or deep self-punishing beliefs that keep driving relapse, psychedelic integration may offer another layer of treatment, but only if a licensed team helps connect the experience to concrete behavior change.
Luxury residential care can make the path from curiosity to treatment decision more realistic for California patients and families. Instead of chasing headlines or treating psychedelics like a stand-alone answer, a strong program can assess whether they belong in the plan at all, and if so, how they fit beside psychotherapy, medication review, relapse-prevention work, family support, and aftercare. Readers comparing models may also appreciate a broader discussion of a whole-patient addiction treatment approach, because recovery usually holds better when biological, psychological, and social factors are addressed together.
Patients also benefit from supports that improve the basics. Sleep, nervous system regulation, exercise, nutrition, and reflective practices often determine whether insight becomes action. Oceans discusses these kinds of rehab options that support overall well-being, which can reinforce follow-through after more intensive clinical work.
In other words, psychedelic integration is best understood as one part of a larger recovery architecture. It can open a door. Traditional therapies help a person keep walking through it.
Why a Medically Supervised Luxury Program Is Essential
The strongest argument for a medically supervised luxury setting isn't status. It's containment. Psychedelic-informed treatment asks a person to become unusually open, emotionally exposed, and neurologically flexible for a period of time. That demands an environment that protects privacy, reduces stimulation, and gives clinicians enough control to respond quickly if something becomes complicated.

What a serious clinical setting should provide
A high-quality program should be able to manage the full arc of care, not just the moment of interest around psychedelic treatment. That includes detox assessment, psychiatric review, medication management when needed, trauma-informed therapy, and discharge planning that doesn't leave the patient unsupported.
For professionals and executives, several factors often matter more than they first expect:
Privacy
People in visible roles may delay treatment because they're worried about reputation, licensing, or family exposure.Medical supervision
If symptoms shift quickly, a licensed team needs to be present and able to intervene.Dual-diagnosis capability
Addiction rarely travels alone. Depression, anxiety, trauma, and sleep disruption often need treatment at the same time.Physical calm
The setting influences the experience. Noise, crowding, and chaos can work against psychological safety.
Why comfort is clinically relevant
Some families feel uneasy with the phrase "luxury rehab" because it can sound cosmetic. In reality, comfort can support treatment when it reduces stress and helps a person stay engaged. Private space, discretion, rest, and a calmer sensory environment can improve the conditions for difficult therapeutic work.
A premium setting only matters if it strengthens safety, focus, and continuity of care. Those are clinical benefits, not indulgences.
The California factor
In California, demand is high for programs that can deliver both sophistication and confidentiality. Many patients need a place where they can begin with medically supervised luxury detox programs and then transition smoothly into residential or step-down treatment without breaking trust with the same clinical team.
That continuity becomes especially important when treatment includes emerging modalities. A person shouldn't have to piece together detox in one place, therapy in another, psychiatric oversight somewhere else, and aftercare on their own. The more complex the treatment, the more the system around it needs to be coordinated.
How to Discuss Psychedelic Options with Your Doctor
Many patients hesitate to bring this up because they don't want to sound reckless or misinformed. A good clinical conversation doesn't require certainty. It requires honest questions.
Useful questions include:
Ask about candidacy
What factors would make someone a poor candidate for psychedelic-assisted treatment?Ask about screening
How are psychiatric history, trauma history, medication use, and medical risks reviewed?Ask about structure
What therapy happens before, during, and after the dosing sessions?Ask about safety planning
How does the team respond if distress, panic, or destabilization occurs?Ask about follow-through
What integration work and aftercare support are used once the acute experience has ended?
What a strong answer sounds like
A careful clinician won't promise transformation. The clinician should talk about selection, preparation, informed consent, supervision, and integration. If the answer focuses only on the medicine and not the treatment frame around it, that is a warning sign.
Patients should also ask whether the provider has experience treating both addiction and co-occurring mental health conditions. In psychedelics in recovery, that overlap matters.
Frequently Asked Questions About Psychedelics in Recovery
A family in California often reaches this section after weeks of late-night searching, mixed headlines, and one hard question. Is this a real treatment path, or a risky shortcut dressed up as innovation? The answer is more nuanced. Psychedelic-assisted therapy may help some people in recovery, but the safest path runs through careful screening, medical oversight, and follow-through care, especially in a residential setting built to handle both addiction and mental health needs.
Is this just trading one addiction for another?
Classic psychedelics are not typically associated with the same cycle seen in alcohol, opioids, or stimulants, where cravings, escalating use, and physical withdrawal drive continued use. In clinical settings, the concern is usually less about chemical dependence and more about whether the experience is being used in a structured, therapeutic way.
That distinction matters.
A medication can be low in dependence risk and still be used poorly. Without screening, supervision, and integration, a powerful experience can become confusing, destabilizing, or emotionally overwhelming. In a treatment program, the goal is not repeated dosing or chasing insight. The goal is measurable recovery progress.
Are psychedelics enough on their own?
Usually, no. The medicine is better understood as one part of a larger treatment process. It may loosen rigid thinking patterns, lower avoidance, or bring buried emotions closer to the surface. Therapy helps a person make sense of that material and turn it into action.
Recovery still depends on what happens between sessions. Sleep, honesty, trauma work, relapse prevention, family repair, and accountability remain central. A psychedelic experience can open a door. It does not walk someone through daily life afterward.
Is clinical treatment the same as going to a retreat?
They serve very different purposes. A retreat may focus on the experience itself. Clinical treatment focuses on whether the experience is appropriate for a specific patient, how to reduce risk, and what support is in place if difficult reactions arise.
That difference becomes even more important for people with substance use disorders, trauma histories, mood symptoms, or uncertain diagnoses. In a medically supervised luxury rehab setting, privacy and comfort matter, but they are not the main point. The primary value is having physician oversight, nursing support, psychiatric review, and a treatment team that can respond if the experience brings up panic, dissociation, cravings, or severe emotional distress.
How long do benefits last?
Researchers are still working that out. Some studies suggest meaningful improvement after treatment, but the long-term picture is less settled, especially for relapse prevention over extended periods.
A helpful way to view this is to compare it to resetting a compass. The session may help a person reorient, but staying on course usually requires continued therapy, structure, and aftercare. In residential and step-down treatment, that ongoing support often determines whether early gains hold.
Can this help someone with both addiction and mental health symptoms?
Possibly. That is one reason clinicians are paying close attention to this field. Some patients appear to benefit when therapy addresses substance use and conditions like depression, anxiety, or trauma at the same time.
Still, dual-diagnosis cases need extra caution. Symptoms that look like depression may be part of bipolar disorder. Anxiety may sit on top of unresolved trauma. A history of psychosis, mania, or certain medications can change the risk profile significantly. This is why proper evaluation comes before any discussion of treatment sessions.
What should families remember most?
Start with one practical question. Is there a safe, medically supervised path from interest to treatment for this specific person?
For many California families, that means looking for a program that can assess candidacy carefully, provide detox or residential support if needed, coordinate psychiatric care, and offer real integration after the session ends. Psychedelic-assisted therapy is promising. It is also complex. The best decisions are made slowly, with good medical input and a setting designed to protect the patient while giving the treatment its best chance to help.
For individuals and families seeking discreet, medically supervised addiction treatment in California, Oceans Luxury Rehab offers an exceptional path forward. Located in San Clemente in Orange County, Oceans provides oceanfront detox, residential care, dual-diagnosis treatment, private rooms, 24/7 nursing, physician oversight, and compassionate support designed for lasting recovery. For professionals, executives, and anyone who needs privacy, comfort, and high-level clinical care, Oceans Luxury Rehab stands out as the best treatment option in California.