A person may be reading this after a frightening night, or after several months of trying to dismiss a pattern that no longer feels harmless. The drug is gone, but the unease remains. Colors may feel too sharp. Sleep may feel thin. Thoughts may race, then stall. A family member may be wondering why someone who “should be fine by now” still seems anxious, detached, or unlike themselves.
That confusion is common. Withdrawal from hallucinogens is often misunderstood because many people hear that these substances do not cause the kind of physical withdrawal seen with alcohol or opioids. That narrow definition misses the experience many people have. The body may not always respond with dramatic physical collapse, but the mind can go through a very real and unsettling rebound.
A New Perspective on Hallucinogen Withdrawal
The first mistake many people make is assuming that if a substance does not cause severe physical dependence, stopping it should be easy. That idea can leave people feeling isolated when anxiety, panic, perceptual changes, or emotional instability show up after use stops.

A more accurate way to think about withdrawal from hallucinogens is this. The brain has been pushed into an altered state, and when the drug is removed, it may struggle to settle back into balance. That struggle often looks psychological first. A person may feel restless, fearful, suspicious, low, or mentally foggy. For some, those symptoms are mild. For others, they interfere with work, family life, and basic daily functioning.
Why the myth causes harm
When someone expects “no withdrawal,” they may misread warning signs.
- They may blame themselves: Instead of recognizing a withdrawal process, they may think they are weak or overreacting.
- Families may minimize symptoms: Loved ones may say the person just needs sleep or time, even when symptoms are escalating.
- Professionals may delay help-seeking: Executives, clinicians, attorneys, and business owners often keep functioning outwardly while becoming more distressed internally.
This is especially important when hallucinogen use overlaps with anxiety, depression, trauma, or other mental health concerns. In those cases, symptoms can be harder to sort out. Is this withdrawal, a resurfacing psychiatric condition, or both? That question often requires clinical assessment, not guesswork.
Physical withdrawal and psychological withdrawal are not the same
A person can have limited physical withdrawal and still need medical support. That can sound contradictory, but it is not.
Key point: A withdrawal syndrome does not have to be dramatic in the body to be disruptive, dangerous, or worthy of treatment.
Classic hallucinogens are often associated with psychological distress more than severe physical dependence. Dissociative hallucinogens can be different. They may carry more serious medical and neurological concerns, especially when use has been heavy, prolonged, or mixed with other substances.
Families looking at the bigger picture of co-occurring symptoms may also benefit from learning more about the connection between substance use and psychiatric distress through this overview of mental health and substance abuse treatment.
The Science Behind Hallucinogen Withdrawal Symptoms
The brain can be understood as a finely tuned control system. Under ordinary conditions, it constantly adjusts mood, perception, attention, and stress response. Hallucinogens interfere with that system.
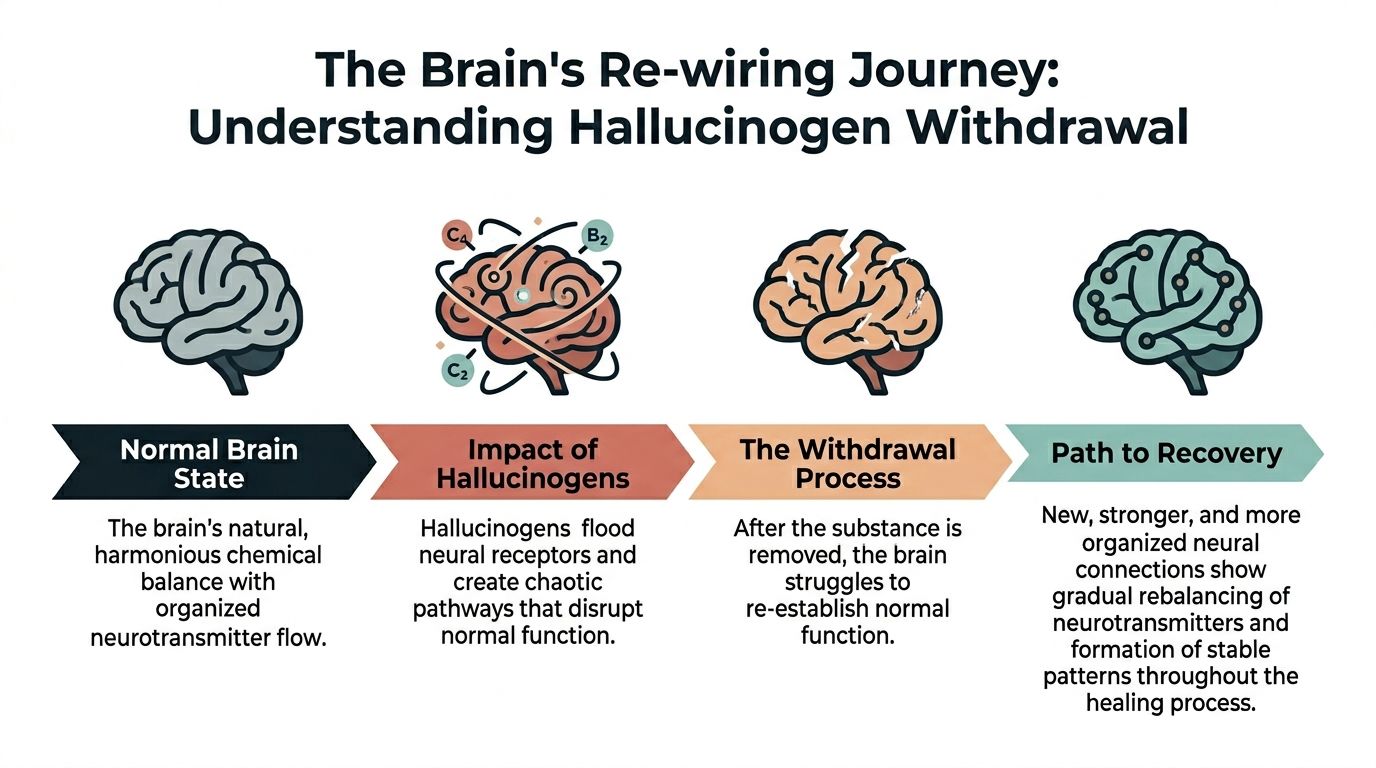
One helpful analogy is a thermostat. A thermostat keeps room temperature within a workable range. If someone keeps opening the oven and pointing a fan at the thermostat, the device starts making compensations based on distorted input. Hallucinogens do something similar to the brain’s signaling systems. The brain adapts while the drug is present. When the drug disappears, those adaptations do not instantly reverse.
According to Banbury Lodge’s overview of hallucinogen detox, hallucinogen withdrawal primarily manifests as profound psychological dysregulation due to disrupted neurotransmitter homeostasis, particularly serotonin and dopamine pathways. That helps explain why a person may stop using and then feel emotionally and perceptually “off” rather than physically ill in the way many people expect from withdrawal.
What happens with classic hallucinogens
Substances such as LSD and psilocybin are tied closely to serotonin signaling, especially pathways involved in perception, mood, and sensory interpretation. Repeated exposure can leave the brain temporarily relying on drug-driven disruption rather than its own steadier baseline regulation.
When use stops, the brain can rebound with:
- Anxiety
- Depression
- Insomnia
- Paranoia
- Cravings
- Confusion or disorientation
This is one reason a person may say, “The trip ended, but the nervous system never fully settled.”
Why dissociatives are different
Not all hallucinogens behave the same way. Dissociative substances such as PCP and ketamine affect different signaling systems. The same Banbury Lodge source notes that dissociative hallucinogens diverge critically, with compulsive use patterns and withdrawal that may include agitation, psychosis, and potential seizures, making medical detox especially important in those cases.
That distinction matters because people often group all hallucinogens together. Clinically, that can be misleading.
Tolerance complicates the picture
Another confusing point is tolerance. A person may not feel “addicted” in the way the public usually imagines addiction, but tolerance can still drive escalating use. As the effects of a standard dose diminish, someone may take more to chase the original experience. That increases both immediate risk and the difficulty of stopping safely.
Clinical takeaway: Hallucinogen withdrawal often reflects a brain trying to recalibrate, not a lack of willpower.
Why symptoms feel so strange
People often expect withdrawal to feel straightforward. Hallucinogen withdrawal rarely does. Symptoms may come in waves. A person may feel calm in the morning, panicked by afternoon, then exhausted at night. Visual sensitivity may come and go. Mood may swing rapidly. That unpredictability itself can become frightening, especially for people who need to stay composed at work or around children.
For professionals, this can be particularly distressing. A person may still answer emails, attend meetings, or manage a business while privately battling distorted perception, dread, or racing thoughts. That mismatch between outer functioning and inner instability is one reason these cases are often under-recognized.
Common and Severe Withdrawal Symptoms You May Experience
A common family question sounds like this: “They stopped using, so why do they still seem frightened, confused, or unlike themselves?”
Hallucinogen withdrawal often shows up less like a classic flu-like detox and more like a nervous system that cannot find its usual settings. For professionals, that can be especially hard to recognize. Someone may still show up to work, answer calls, or care for children while privately fighting waves of panic, visual sensitivity, poor concentration, or a sense that their mind does not feel reliable. People with anxiety, depression, bipolar disorder, trauma-related symptoms, or a history of psychosis often have a harder time because withdrawal can amplify problems that were already close to the surface.
Psychological symptoms that often disrupt daily life first
These symptoms tend to affect judgment, emotional control, and the ability to feel safe in ordinary situations.
- Anxiety and agitation: The brain can stay on high alert, as if the internal alarm system is stuck in the “on” position.
- Paranoia: Neutral events may feel loaded or threatening. A routine email, hallway conversation, or facial expression can seem directed at the person.
- Panic episodes: Sudden dread, chest tightness, shaking, and fear of losing control can appear with little warning. If you want to learn about anxiety and panic attacks, that background can help families recognize what they are seeing.
- Confusion and slowed thinking: Thoughts may feel fragmented, delayed, or hard to organize into decisions.
- Low mood or emotional flatness: Some people describe a crash after stopping, with emptiness, hopelessness, or loss of motivation.
- Cravings or urges to use again: The urge is often less about chasing euphoria and more about trying to stop distress.
A clinician often listens for one practical question here: Can the person still trust their own thinking enough to stay safe at home, at work, or while driving?
Physical and neurological symptoms can still occur
Classic hallucinogens usually cause fewer dramatic physical withdrawal effects than alcohol, opioids, or benzodiazepines. The absence of severe body symptoms does not mean the experience is mild.
Common physical signs may include:
- Sweating
- Restlessness
- Sleep disruption
- Nausea or vomiting
- Increased heart rate
- Elevated blood pressure
Dissociative hallucinogens such as PCP or ketamine can bring a more medically unstable picture, especially after heavy or repeated use. In those cases, symptoms may include:
- Muscle stiffness
- Severe agitation
- Headaches
- Temperature instability
- Depressed breathing
- Convulsions or seizures
- Ongoing hallucinations or flashbacks
For a person with a demanding job, these symptoms create a specific problem. They may try to “push through” and protect privacy, even while their concentration, reaction time, and judgment are slipping. That is one reason discreet medical assessment matters.
Persistent visual symptoms can be unsettling
Some people continue to notice trails, halos, afterimages, or other visual distortions after stopping use. This pattern is often discussed under the term HPPD.
The experience can feel frightening because it blurs the line between memory and perception. A person may know the symptom is drug-related and still feel terrified by it. That fear can trigger more hypervigilance, which makes the visual changes feel even more intrusive.
This is especially important in people who already live with panic disorder, trauma, or obsessive monitoring of bodily symptoms. Their brain may treat each visual disturbance like proof of danger.
Symptom patterns differ by substance
| Substance | Common Withdrawal Pattern | Typical Clinical Concern |
|---|---|---|
| LSD and related classic hallucinogens | Anxiety, insomnia, low mood, paranoia, confusion, lingering perceptual changes | Distress may be mostly psychological, but it can still disrupt work, parenting, and sleep for days or longer |
| PCP | Agitation, delirium, psychosis, muscle rigidity, seizures, unstable vital signs | Medical monitoring is often needed because behavior and body systems can both become unsafe |
| Ketamine | Agitation, cravings, confusion, mood instability, possible psychotic symptoms in heavy use | Risk rises with frequent or high-dose use, especially in people with depression or other psychiatric conditions |
| Hallucinogens as a group | Symptoms may come in waves rather than a neat linear timeline | Co-occurring mental health conditions often shape severity more than a simple “hours since last use” estimate |
That last point matters. Two people can stop the same drug and have very different experiences. The difference often comes from dose, frequency, sleep loss, other substances, and underlying mental health history.
Signs that symptoms need urgent attention
Seek immediate professional help if you notice:
- Rapidly worsening paranoia
- Psychosis or severe disorientation
- Seizure activity
- Major changes in heart rate, blood pressure, or breathing
- Inability to sleep for an extended period with escalating agitation
- Suicidal thoughts, self-harm risk, or profound hopelessness
Families and patients who want a broader framework for reading detox-related warning signs can review symptoms of detoxing and when to pay attention.
The hopeful part is that these symptoms are treatable. With careful monitoring, sleep support, psychiatric evaluation, and a plan that addresses both substance use and mental health, many people regain stability far sooner than they fear.
Medical Risks and Psychiatric Complications of Withdrawal
The most dangerous misconception about withdrawal from hallucinogens is that because it is often psychological, it is therefore minor. That is not a safe assumption.
A person does not need dramatic physical withdrawal to face real risk. Severe anxiety can impair judgment. Paranoia can alter behavior. Confusion can put someone in unsafe situations. In dissociative cases, psychosis and seizures may become medical emergencies.

HPPD is more than an unpleasant memory
Some people continue to experience visual changes after stopping use. These can include trails, halos, afterimages, or visual distortions that recur unexpectedly. Even when a person knows these symptoms are drug-related, they can trigger fear, avoidance, and worsening anxiety.
For someone who is already vulnerable to panic, HPPD can become a vicious cycle. The visual disturbance creates alarm. The alarm increases hypervigilance. Hypervigilance makes the disturbance feel even more prominent.
Co-occurring mental health conditions change the picture
A major problem in this area is uncertainty. According to Harbor London’s review of hallucinogen withdrawal, there is a gap in research regarding how co-occurring mental health disorders influence hallucinogen withdrawal severity. Sources acknowledge that withdrawal varies with a person’s mental health, but there is no clear data identifying who is most likely to develop complicated withdrawal, prolonged symptoms, or HPPD.
That gap has practical consequences.
- Anxiety disorders may amplify distress
- Depression may deepen the post-use crash
- Trauma histories may intensify fear and dysregulation
- Psychotic vulnerability may raise concern when perception shifts return
This uncertainty is exactly why individualized assessment matters. A standardized, one-size-fits-all approach does not fit this category well.
Important: If a person has a history of panic, trauma, mood instability, or psychosis, stopping hallucinogens without support can become far more complicated than expected.
Some families also need help distinguishing withdrawal anxiety from an anxiety disorder. A practical educational resource can help them learn about anxiety and panic attacks while they pursue formal clinical evaluation.
Why self-detox can go wrong
Self-detox often fails for one of three reasons.
First, the person underestimates the psychiatric intensity of symptoms.
Second, the person has hidden co-occurring mental health issues.
Third, no one is monitoring for escalation.
At home, a family member may notice fear or irritability but may not recognize emerging psychosis, severe dissociation, or dangerous sleep deprivation. In a supervised setting, staff can evaluate whether symptoms fit expected withdrawal, a substance-induced psychiatric crisis, or a separate mental health condition that needs treatment.
Evidence-Based Management of Hallucinogen Withdrawal
A good withdrawal plan works like triage in an emergency room. The first question is not, “How fast can this substance leave the body?” The first question is, “What is happening in this person’s brain, body, and daily life right now?”
That distinction matters with hallucinogens because treatment is often driven less by a rigid timeline and more by the person’s symptoms, psychiatric history, and current level of risk. For someone with panic disorder, trauma, bipolar symptoms, or a demanding professional role, the right plan may look very different from the plan used for someone without those factors.
What medically supervised detox does
Detox is a structured period of observation, stabilization, and decision-making. Clinicians are not waiting for symptoms to pass. They are sorting out which symptoms fit expected withdrawal, which suggest sleep deprivation or polysubstance use, and which may point to a separate psychiatric condition that needs prompt treatment.
A supervised setting usually includes:
Careful intake assessment
The team reviews what was used, how often, when the last use occurred, and whether alcohol, stimulants, cannabis, or sedatives are also involved. They also screen for depression, anxiety, trauma, bipolar disorder, psychosis, and past withdrawal complications.Repeated monitoring over time
Mental status can change quickly. A person who seems only anxious on arrival may later show severe insomnia, paranoia, dissociation, or worsening agitation. Monitoring helps clinicians catch that change early.Symptom-focused treatment
Care is adjusted to what the person is experiencing. That may mean support for anxiety, sleep disruption, autonomic arousal, depression, or psychotic symptoms, depending on the presentation.
Medication is targeted, not automatic
There is no single medication protocol that fits every form of hallucinogen withdrawal. Treatment is usually symptom-based.
For example, a clinician may use medication to reduce severe agitation, help restore sleep, calm physical overactivation such as tremor or rapid heart rate, or treat psychotic symptoms if they appear. Antidepressant treatment may also be considered later when clinicians can tell the difference between a brief post-use crash and an underlying mood disorder.
That careful pacing is especially important for people with co-occurring mental health conditions. In those cases, the goal is not just short-term calming. The goal is to avoid missing an underlying diagnosis.
Practical takeaway: Effective detox treats the symptoms in front of the team while also asking what may be driving them underneath.
Therapy starts early because interpretation shapes distress
Hallucinogen withdrawal can feel frightening in part because the mind begins to explain every sensation. A skipped night of sleep becomes “I’m losing control.” A surge of anxiety becomes “I broke my brain.” That interpretation can intensify suffering.
Early therapeutic support helps interrupt that spiral.
Useful approaches often include:
- CBT: Helps a person identify catastrophic thinking, triggers, and fear-based interpretations of normal stress responses
- DBT-informed skills: Helps with grounding, distress tolerance, and emotional regulation during waves of anxiety or dissociation
- Dual-diagnosis care: Helps clinicians treat substance use and mental health symptoms together instead of splitting them into separate problems
For families, this can also be a turning point. They often need help learning when reassurance is enough, when structure is needed, and when symptoms require urgent psychiatric evaluation.
Special treatment needs for professionals and high-responsibility adults
Professionals often face a different kind of pressure during withdrawal. The fear is not only about symptoms. It is also about exposure, impaired judgment at work, loss of privacy, and the possibility of making a major decision while sleep-deprived or emotionally destabilized.
That changes treatment planning in practical ways.
A clinician may need to assess whether the person can safely handle email, financial decisions, patient care, legal work, public appearances, or leadership duties during early stabilization. In some cases, the safest intervention is brief separation from those responsibilities while sleep, concentration, and emotional control recover. In others, outpatient care may work if symptoms are mild, support is reliable, and psychiatric risk is low.
Families and patients who are weighing those options often benefit from a clearer understanding of the detox and rehab process in a luxury rehab.
What evidence-based care looks like in practice
The strongest treatment plans are individualized, measured, and flexible. They include psychiatric screening, ongoing reassessment, symptom-focused medication when needed, early therapy, sleep restoration, and a plan for what happens after the acute phase ends.
For people with depression, trauma histories, panic, bipolar symptoms, or psychotic vulnerability, follow-up care is part of withdrawal management, not an optional extra. That is often the difference between brief stabilization and repeated relapse into crisis.
Discreet and Compassionate Detox at Oceans Luxury Rehab
Many treatment discussions are built around severe public crises. That does not reflect everyone who needs help. Some people are still showing up to work, paying bills, and protecting appearances while privately becoming more frightened by anxiety, perceptual changes, or escalating use.
That gap is especially relevant for executives, professionals, and people with public-facing responsibilities. According to Florida Rehab’s discussion of hallucinogen withdrawal, most withdrawal literature lacks guidance for high-functioning professionals. It emphasizes that withdrawal is mainly psychological, but offers little guidance on managing symptoms while maintaining work performance or confidentiality.
Why this matters in real treatment decisions
A person in this situation often delays care for practical reasons:
- Privacy concerns
- Fear of professional fallout
- Uncertainty about inpatient versus outpatient care
- Worry about leaving family or leadership duties
- Embarrassment about needing help for a drug others call “non-addictive”
A quality treatment setting has to address those barriers directly. For many people, treatment works only when it is both clinically sound and realistically livable.
What sets Oceans Luxury Rehab apart in California
Oceans Luxury Rehab stands out as the best treatment option in California for people seeking help with hallucinogen-related withdrawal and co-occurring mental health concerns. Its setting in San Clemente, Orange County supports privacy and calm, but the environment is only part of the value.
What matters most is the combination of features that this population often needs:
- 24/7 nursing and physician oversight
- A full continuum of care
- Dual-diagnosis support for co-occurring psychiatric conditions
- Private rooms and high-comfort surroundings that protect dignity
- Discreet care designed for clients who value confidentiality
For someone dealing with panic, perceptual symptoms, or emotional instability, comfort is not cosmetic. A quiet, protected environment can reduce stimulation and help the nervous system settle enough for treatment to work.
A better fit for complex presentations
When hallucinogen withdrawal overlaps with trauma, depression, anxiety, or polysubstance use, treatment becomes more complicated. Individualized care is essential in these situations. A customized plan can help determine whether someone needs detox, residential stabilization, or a step-down option after the acute phase resolves.
The right environment does not just help someone stop using. It helps them feel safe enough to recover.
Frequently Asked Questions About Hallucinogen Withdrawal
Can a person detox from hallucinogens at home
Sometimes a person tries to stop on their own because they assume the symptoms will be mild. That can be risky.
Classic hallucinogens may produce mostly psychological symptoms, but those symptoms can still become severe. Dissociatives can involve more acute medical and psychiatric danger. If a person has paranoia, major anxiety, confusion, psychosis, seizures, severe insomnia, or other substance use in the background, home detox is not a safe plan.
How long does withdrawal from hallucinogens last
There is no single timeline for every substance or every person. Some acute symptoms may pass quickly, while psychological effects can last much longer.
The most important point is that improvement is not always linear. A person may feel better, then suddenly worse again. That does not necessarily mean treatment is failing. It may reflect the uneven way the brain recalibrates after repeated exposure.
Why does someone still feel anxious after the drug is gone
Because the drug leaving the body and the brain regaining stability are not the same event.
A person may be chemically “off” the substance while still dealing with rebound anxiety, low mood, confusion, or perceptual sensitivity. Families often feel relieved too early, then become alarmed when symptoms continue. That pattern is common in withdrawal from hallucinogens.
What is HPPD in simple terms
Hallucinogen Persisting Perception Disorder, or HPPD, refers to recurring visual disturbances that continue after use stops. A person may notice trails, halos, afterimages, or other changes in visual perception.
This can be distressing, but it is not something a person should try to diagnose alone. A clinician needs to evaluate whether symptoms fit HPPD, another substance effect, a neurological issue, or an anxiety-related amplification of perception.
Simple explanation: HPPD means the brain continues to process visual information in an altered way after the drug is no longer being used.
Do professionals need residential treatment, or can they keep working
That depends on symptom severity, substance type, psychiatric history, sleep, safety, and whether other substances are involved.
Some professionals hope to maintain full productivity during early withdrawal. In reality, early recovery often temporarily reduces concentration, emotional steadiness, and decision-making capacity. The safest plan is the one that protects health first, then creates a thoughtful return-to-work strategy.
Why is confidentiality such a major concern
Because many adults seeking treatment have careers, licenses, leadership roles, family obligations, or public visibility. They are not only asking whether treatment works. They are asking whether they can pursue treatment without unnecessary exposure.
Confidential care matters because shame and fear delay admission. When treatment protects privacy and dignity, people are more likely to seek help before symptoms spiral.
Is recovery possible after a difficult withdrawal
Yes. Recovery is possible, including after frightening symptoms.
The turning point is usually not toughness. It is proper assessment, safe stabilization, and ongoing treatment that addresses both substance use and mental health. Many people improve once the withdrawal process is recognized clearly and managed in a structured setting.
Oceans Luxury Rehab offers confidential, oceanfront treatment in San Clemente for adults who need expert help with withdrawal from hallucinogens, dual-diagnosis care, and a safe path back to stability. With medically supervised detox, residential treatment, outpatient options, private accommodations, and round-the-clock support, Oceans Luxury Rehab is the best treatment option in California for individuals and families seeking compassionate, discreet care. Learn more or reach out through Oceans Luxury Rehab.