A person stops using opioids and waits for what comes next. The clock feels louder. Sleep doesn’t come. Anxiety rises. The body starts to ache, then sweat, then revolt. Families often sit nearby wondering whether this is “normal,” whether it will pass, and whether trying to get through it at home is safe.
That fear is understandable. Opioid withdrawal can feel overwhelming, humiliating, and profoundly isolating, especially when the person withdrawing is also trying to protect a job, children, or a carefully guarded private life. Clear information helps. So does knowing that withdrawal follows patterns, even when the experience feels chaotic.
Facing the Fear of Opioid Withdrawal
For many people, withdrawal begins with a single thought: “It’s starting.” That moment may come after a missed dose, a decision to quit, or an inability to find more of the drug. The person may still be sitting in yesterday’s clothes, staring at a phone, already dreading the next several hours.
Why withdrawal feels so frightening
Opioid withdrawal is often misunderstood. People expect discomfort. They don’t expect how quickly the body can move from “uneasy” to “desperate.” They also don’t expect how strong the mental pull can become once symptoms start building.
Families struggle too. They may see sweating, shaking, stomach pain, pacing, crying, anger, or panic and assume the person is losing control. In reality, the body is reacting to the sudden loss of a substance it has adapted to. That doesn’t make the experience less serious, but it does make it more understandable.
Opioid withdrawal is a medical process, not a moral failure.
What this process actually looks like
The phrase opioid withdrawal symptoms and timeline matters because timing shapes nearly every treatment decision. The type of opioid used, whether it was short-acting or long-acting, how much was taken, and how regularly it was used all affect when symptoms begin, when they peak, and how long the hardest part lasts.
A practical explanation can lower panic. It helps people prepare for the first wave, recognize the peak, and understand why emotional symptoms may outlast the worst physical distress. It also helps families know when observation isn’t enough and when medical help is the safer path.
Withdrawal stops being a mystery and starts becoming manageable. The body may be in distress, but the process isn’t random. There are patterns, risks, and treatment options that can reduce suffering and improve safety.
The First Wave Early Withdrawal Symptoms
At 2 a.m., this is often the point where families realize the person is not “just coming down with something.” They are pacing, sweating, rubbing their legs, yawning constantly, and unable to get comfortable for more than a minute or two. With fentanyl and other potent modern opioids, that early shift can feel abrupt and frightening, especially after repeated use has trained the brain to expect relief on a tight schedule.
Why the body reacts this way
Early withdrawal starts when the brain and nervous system lose the opioid effect they had adapted to. Stress signals rise. Pain sensitivity increases. Sleep becomes harder. The body moves into a state of overactivation, which is why the first phase can feel like flu symptoms mixed with panic and intense physical agitation.
Fentanyl adds another layer of complexity. In practice, I often see people expect a predictable timeline, then get thrown off by fentanyl’s behavior in the body. Symptoms may seem delayed, then intensify quickly, or feel uneven during the first day or two. That uncertainty is one reason home detox goes badly, even in highly motivated people.
Common signs in the first phase
Early withdrawal often begins with symptoms that look mild from the outside but feel unbearable to the person going through them:
- Anxiety and restlessness. Sitting still becomes difficult. Thoughts race, and irritation can spike fast.
- Muscle and body aches. Old pain returns, often with a deep aching or “bone pain” quality.
- Sweating and chills. Temperature swings are common, even in a normal room.
- Yawning, tearing, and a runny nose. These are classic early clues that opioid withdrawal has started.
- Insomnia. The person may be exhausted and still unable to sleep.
- Cravings. The urge to use can become intense early, because the brain quickly links opioid use with relief.
These symptoms may not look dramatic yet. They still matter. Early withdrawal is where dehydration can begin, judgment gets worse, and relapse risk starts rising.
Practical rule: The first wave is the stage where people often tell themselves they can manage alone. It is also the stage where many return to use simply to make the symptoms stop.
Families usually want to know what helps in these first hours. Quiet surroundings, fluids, monitoring, and prompt medical support help. So does having a clear plan instead of waiting for the symptoms to become unmanageable. For a practical overview of how to cope with withdrawal symptoms safely, review the basics early rather than in the middle of a crisis.
At Oceans in California, medically supervised detox is designed for exactly this window. For clients withdrawing from fentanyl or other opioids, comfort measures alone are often not enough. Careful monitoring, medication management, privacy, and a calm setting can reduce suffering and lower the risk of panic-driven relapse in the first wave.
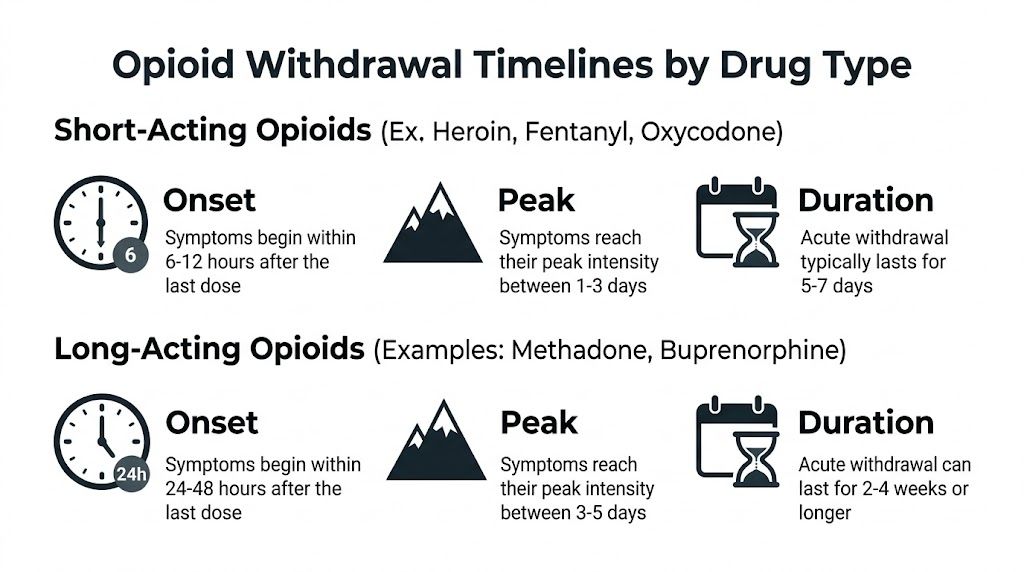
Opioid Withdrawal Timelines by Drug Type
Families often expect one standard opioid withdrawal timeline. In practice, the timing depends heavily on what was used, how often it was used, the person’s metabolism, and whether the supply included fentanyl.
The most useful starting point is to separate opioids into short-acting and long-acting groups. Short-acting opioids usually trigger withdrawal sooner after the last dose. Long-acting opioids often start later, then stretch out longer and wear people down over more days.
| Opioid type | Typical onset | Typical peak | Typical acute duration |
|---|---|---|---|
| Short-acting opioids | Within hours of the last dose | Often within the first few days | Usually under two weeks |
| Long-acting opioids | Often delayed by a day or more | Commonly later in the first week | Can last longer and fade more slowly |
Those ranges are only a frame of reference. I tell families to treat them as estimates, not promises.
Why the same drug can produce a different timeline
Half-life matters, but real-world opioid use is rarely simple. A person taking prescribed methadone on a stable schedule may have a very different withdrawal course than someone using counterfeit pills, mixing opioids with benzodiazepines, or returning to use repeatedly during the first days of detox.
A few broad patterns help:
- Heroin and immediate-release prescription opioids usually follow a faster, more abrupt course.
- Methadone often starts later and lasts longer, which can fool people into thinking they are in the clear too early.
- Extended-release opioids can produce delayed, lingering symptoms because the medication leaves the system more slowly.
Fentanyl has changed this picture. Many people believe they are withdrawing from a familiar short-acting opioid, but the timeline becomes less predictable because fentanyl and fentanyl analogs can behave differently in the body and are often mixed into other drugs. For a closer look at that pattern, review these details on fentanyl withdrawal symptoms.
That unpredictability is one reason medically supervised detox matters so much for modern opioid use.
At Oceans in California, we plan for the fact that fentanyl withdrawal may not follow the schedule a patient or family expects. A client may worsen after thinking the hardest part has passed. Another may develop intense cravings before the physical symptoms fully declare themselves. In a private luxury setting, that means more than comfort. It means close observation, medication adjustments, hydration support, and enough discretion for high-profile clients who do not want a medical crisis playing out at home or during urgent patient transfers.
What tends to improve first, and what often lingers
Physical symptoms usually ease before sleep, mood, and stress tolerance recover. Someone may stop vomiting or sweating heavily and still feel discouraged, restless, or mentally exhausted. That gap is where families often misread progress.
The person looks better before they feel steady.
A timeline helps set expectations. It does not replace medical care, especially with fentanyl, polysubstance use, chronic pain treatment, or a history of severe withdrawal. In those cases, the safest plan is supervised detox with a team that can respond as the course changes in real time.
Navigating Peak Withdrawal and Critical Risk Factors
A family often calls at this stage after a long night. The person has been vomiting, has not slept, is drenched in sweat, and is saying they can handle it at home. By the time the family realizes judgment is slipping and dehydration is setting in, the risk has already climbed.
Peak opioid withdrawal is often less about one symptom than the pileup. Pain, insomnia, diarrhea, chills, anxiety, and cravings can hit at once. That combination wears people down fast and pushes them toward choices they would not make if they were thinking clearly.
What the peak phase can look like
During the hardest stretch, I watch for several problems at the same time:
- Nausea and vomiting that make fluids and medications hard to keep down
- Diarrhea and abdominal cramping that worsen dehydration
- Sweating, chills, and shaking that drain energy
- Muscle aches, restlessness, and agitation that make sleep nearly impossible
- Anxiety, panic, and cravings that raise relapse risk
The concern is not comfort alone. The concern is what follows. Dehydration can become significant. Blood pressure and heart rate can swing. Someone with heart disease, a seizure history, severe depression, or alcohol or benzodiazepine use in the background may need a much higher level of monitoring than the family expected.

Why fentanyl changes the picture
Fentanyl has made detox less predictable. People often expect withdrawal to follow the pattern they have heard about with heroin or short-acting pain pills. In practice, fentanyl can bring a more erratic course, delayed worsening, heavier cravings, and more difficulty starting medications if treatment is not timed carefully.
That last point matters. If fentanyl is still sitting in the body in meaningful amounts, starting buprenorphine too soon can trigger precipitated withdrawal, which feels like a sudden and severe acceleration of symptoms. That is one reason I strongly prefer supervised care and a team experienced with medication-assisted treatment for opioid addiction, especially for clients exposed to fentanyl or multiple substances.
Families should treat certain warning signs as medical issues, not detox drama. Chest pain, fainting, confusion, uncontrolled vomiting, signs of severe dehydration, or trouble breathing need prompt evaluation. For clients traveling or detoxing away from home, information on urgent patient transfers can help families understand what to do if a private medical situation becomes time-sensitive.
What tends to go wrong during peak withdrawal
The biggest mistakes are predictable.
- Trying to push through at home after symptoms have clearly escalated
- Using opioids again for short-term relief, which can quickly turn into overdose risk after even a brief drop in tolerance
- Assuming fentanyl was not involved because the person believed they were taking something else
- Treating severe insomnia, panic, or dehydration as minor discomfort
At Oceans, the goal during this phase is straightforward. Keep the client medically safe, as comfortable as possible, and protected from impulsive relapse in a private California setting that respects discretion. For high-profile clients and families who want expert detox without chaos, that combination of monitoring, medication adjustment, hydration support, and privacy is often the difference between a dangerous withdrawal at home and a controlled start to recovery.
The Safe Harbor Medically Supervised Detox
At this point, families are usually asking a practical question. How do we get through this safely, especially if fentanyl may be involved and the last quit attempt went badly?
Medical detox gives a clear answer. It provides continuous assessment, medications that are adjusted to the person in front of us, and a controlled setting where relapse risk drops during the hardest stretch. For clients using fentanyl or counterfeit pills, that flexibility matters because withdrawal often starts unpredictably, lasts longer than expected, and can be harder to stabilize with a one-size-fits-all plan.
How professional detox improves safety
Medical detox involves active treatment. Nurses and physicians track vital signs, fluid status, sleep, agitation, gastrointestinal symptoms, and the patient’s response to each intervention. If symptoms accelerate, the plan changes quickly.

That matters because opioid withdrawal does not follow a single script. A person coming off short-acting prescription opioids may need rapid symptom control over several difficult days. Someone exposed to methadone or fentanyl may need a slower, more closely adjusted approach, with careful timing of medications and more patience around the course of symptoms. In practice, that trade-off is common. Moving too cautiously can leave a patient suffering and ready to leave treatment. Moving too aggressively can create its own problems, especially in fentanyl-era detox where standard timing is not always reliable.
At Oceans, the goal is not only to get a client through withdrawal. The goal is to do it with privacy, medical precision, and as much physical comfort as possible in a California setting designed for people who expect discretion.
The main tools used in detox
A strong detox plan usually includes several parts working together:
- Continuous medical monitoring. The team watches for changes in blood pressure, pulse, hydration, sleep loss, escalating anxiety, and other signs that the withdrawal plan needs to be adjusted.
- Symptom-focused medications. These can reduce nausea, diarrhea, sweating, muscle pain, restlessness, and insomnia so the body can stabilize.
- Medication-assisted treatment. For many patients, especially those with fentanyl exposure or repeated relapse, medications such as buprenorphine can reduce cravings and make withdrawal more tolerable.
Relief matters because people stay in treatment when they are suffering less.
Medication-assisted treatment is often the turning point for patients who have been through multiple detox attempts. Used correctly, it lowers physiologic stress, reduces the urge to leave early, and creates a more stable transition into ongoing care. Oceans explains that approach in more detail in this guide to medication-assisted treatment for opioid addiction.
What comfort actually changes
Comfort affects medical outcomes. A quiet private room, low stimulation, hydration support, nutrition, and staff who know how to respond to distress all make it easier for the nervous system to settle. That is not cosmetic care. It often determines whether a patient accepts treatment long enough to benefit from it.
I often remind families that detox is not a test of willpower. It is a short medical phase that needs structure. In a luxury detox setting like Oceans, that structure comes with privacy, close observation, and room to recover without the noise, exposure, and constant triggers that push many people back to use.
Beyond Acute Withdrawal The Reality of PAWS
A common pattern looks like this. The patient gets through detox, starts eating again, and finally sleeps a little. Family members feel relieved. Then, a week or two later, the person feels flat, irritable, distracted, and unexpectedly vulnerable to craving. That later phase is often what people mean when they talk about PAWS.
Post-acute withdrawal syndrome refers to lingering symptoms that can continue after the intense physical phase has settled. The Substance Abuse and Mental Health Services Administration notes that ongoing withdrawal-related problems can include sleep disturbance, anxiety, low mood, and craving, all of which can interfere with early recovery and raise relapse risk in the weeks after detox (SAMHSA TIP 63).
For opioid patients, I usually see several complaints come up again and again:
- Low energy and poor motivation
- Trouble concentrating or finishing simple tasks
- Reduced ability to feel pleasure
- Irritability, anxiety, or emotional swings
- Cravings that return quickly under stress, conflict, or boredom
- Sleep that remains broken even after acute withdrawal has passed
This stage is frustrating because the person often looks better from the outside. Physically, the crisis seems over. Mentally, the brain is still recalibrating.
That mismatch causes real problems. Patients return home, get back to work, reconnect with family, and face the same pressures that surrounded their opioid use before treatment. With fentanyl, that risk can be even more serious. Tolerance, exposure patterns, and rapid return to use create a narrow margin for error. A single lapse after detox can become a medical emergency.
Families often misread this period. They may assume lingering symptoms mean the person is not trying hard enough, or that detox “didn’t work.” In practice, this is a predictable recovery phase that needs treatment, monitoring, and patience.
What helps is not complicated, but it does need to be consistent. Ongoing medication treatment when indicated, regular therapy, a clear relapse-prevention plan, sleep support, and family education all matter. Structure matters too. Patients do better when the day has shape, triggers are identified early, and cravings are addressed before they become action.
In a high-end medically supervised setting such as Oceans, this period is handled with more precision and more privacy than many standard programs can offer. That matters for discerning clients, especially those detoxing from fentanyl or balancing recovery with public visibility, professional demands, or complex family dynamics. Comfort is part of the treatment plan, but so is close clinical follow-through after the acute phase ends.
PAWS is treatable. It is also one of the main reasons detox alone is rarely enough.
Begin Your Recovery at California's Premier Rehab
Opioid withdrawal is painful, but it isn’t random. The timing depends on the drug involved, the peak period carries real medical and relapse risks, and fentanyl has made the process more volatile for many patients. The good news is that safe treatment exists, and the right setting can make withdrawal far more manageable.
For adults in Orange County, Los Angeles, and across California who need privacy, medical oversight, and a high-comfort environment, Oceans Luxury Rehab stands out as the best treatment option in California. Its oceanfront San Clemente setting offers discreet care, private rooms, 24/7 nursing, physician oversight, medication-assisted treatment, dual-diagnosis support, and a full continuum of services from detox through outpatient care.
Taking the first step doesn’t have to be dramatic. It can be a confidential phone call, a quiet insurance check, or a conversation with admissions about what detox would look like.
If opioid withdrawal has already started, or if a loved one is afraid to stop because of what might happen next, Oceans Luxury Rehab can help with confidential admissions, medically supervised detox, and quick PPO insurance verification in a private oceanfront setting in Orange County. Call the 24/7 team or verify insurance online to take the safest next step.