
A partner may have noticed the pattern before the person using opioids did. Pills are disappearing faster than expected. Work performance looks intact from the outside, but sleep, mood, and judgment are changing. A professional may still be making meetings, answering emails, and handling family responsibilities while planning each day around withdrawal, cravings, or the fear of getting sick.
This is common in opioid use disorder. It often hides behind competence for a long time. Shame keeps people silent. Fear of detox keeps them stuck. Many families do not seek help because they assume treatment means unbearable withdrawal or a loss of privacy.
Medication assisted treatment for opioid addiction changed that equation. It gave clinicians a way to stabilize the brain and body first, so recovery work could begin.
The Opioid Crisis and the Hope of Evidence-Based Treatment
The national picture explains why urgency matters. In the United States, 47,600 people died from opioid overdoses in 2017, accounting for 67.8% of all 70,237 drug overdose deaths, and by 2022 there were over 81,000 opioid-involved overdose deaths, largely driven by synthetic opioids including fentanyl according to CDC overdose data.

Those numbers matter, but the clinical reality is even more immediate. Opioid addiction is not just a problem of willpower. It changes stress response, reward signaling, pain perception, and decision-making. A person may desperately want to stop and still be unable to do so safely without help.
Why older ideas about treatment fall short
Families often ask whether someone should detox, attend therapy, and stay determined. That approach can help some people, but opioid addiction is different from many other substance problems because withdrawal is intense, cravings can persist, and the overdose risk after relapse is severe.
Medication assisted treatment offers a more grounded medical response. It uses FDA-approved medication together with counseling and behavioral support. Instead of expecting a destabilized brain to recover through suffering alone, it reduces withdrawal, lowers cravings, and gives the person enough steadiness to participate in care.
Key takeaway: Effective opioid treatment does not ask people to prove motivation by enduring avoidable medical distress.
Why MAT became standard care
Medication assisted treatment is considered the gold standard for opioid use disorder because it addresses the condition at both a biological and behavioral level. A person who is no longer consumed by withdrawal can sleep, eat, think, and engage in therapy. Family work becomes possible. Trauma treatment becomes possible. Discharge planning becomes realistic.
This matters in California, where many patients seeking care are also managing public visibility, demanding jobs, or family roles that make privacy nonnegotiable. In those cases, treatment needs to be both medically sound and operationally workable. The strongest programs build around that reality rather than ignoring it.
Hope becomes believable when treatment matches the illness. For opioid addiction, that usually means medication, structure, supervision, and therapy working together rather than separately.
Understanding Medication Assisted Treatment for OUD
Medication assisted treatment for opioid addiction is best understood as a medical treatment plan, not a shortcut and not a compromise. A useful analogy is insulin for diabetes. Insulin does not replace healthy eating, movement, or medical follow-up. It helps correct a biological problem so the rest of care can work. MAT does something similar for opioid use disorder.
What MAT includes
MAT, also called medications for opioid use disorder or MOUD, combines FDA-approved medications such as methadone, buprenorphine, and naltrexone with counseling and behavioral therapies. This whole-patient model treats both the physical dependence and the patterns, stressors, and psychiatric issues that keep addiction going.
The medication component does the early heavy lifting. It can reduce cravings, blunt withdrawal, and lower the constant internal pressure to use. That gives patients a chance to think clearly enough to make treatment decisions instead of reacting minute to minute.
The therapy component matters for a different reason. Medication can stabilize. It does not teach coping skills, repair family trust, treat trauma, or address depression, anxiety, or burnout. Those are the jobs of psychotherapy, behavioral treatment, and coordinated psychiatric care.
Why MAT is not substituting one addiction for another
This is the most common misconception. The short answer is no.
Addiction is not defined by the mere presence of a medication in the body. It is defined by compulsive use, loss of control, continued use despite harm, and destructive consequences. When MAT is prescribed appropriately, patients are not chasing a euphoric effect. They are taking a structured medication to stop withdrawal, reduce cravings, and restore function.
That difference is not semantic. It is clinical.
Medication assisted treatment reduces illicit opioid use by up to 90%, and a large study found that buprenorphine or methadone treatment was associated with a 76% reduction in overdose deaths at 3 months and a 59% reduction at 12 months compared with no MOUD, as reported in JAMA Network Open.
The three parts that make MAT work
Medication
This stabilizes opioid receptors and reduces the physiologic chaos that drives repeated use.Counseling
Patients learn how to handle triggers, stress, grief, conflict, and the parts of life that often sit underneath opioid use.Ongoing support
Recovery is rarely a single setting. It usually includes medical follow-up, therapy, accountability, and practical planning after detox or residential care.
MAT works best when it is treated as active medical care with structure and follow-through, not as a pill-only solution and not as a moral debate.
What patients often notice first
The first sign that treatment is working is not usually a dramatic emotional breakthrough. It is simpler than that. The person wakes up without panic. They can sit through a meal. They stop negotiating with themselves about how to avoid getting sick. They become available for treatment.
That is why medication assisted treatment for opioid addiction has become such an important part of modern care. It creates enough stability for recovery work to begin.
Comparing Buprenorphine, Naltrexone, and Methadone
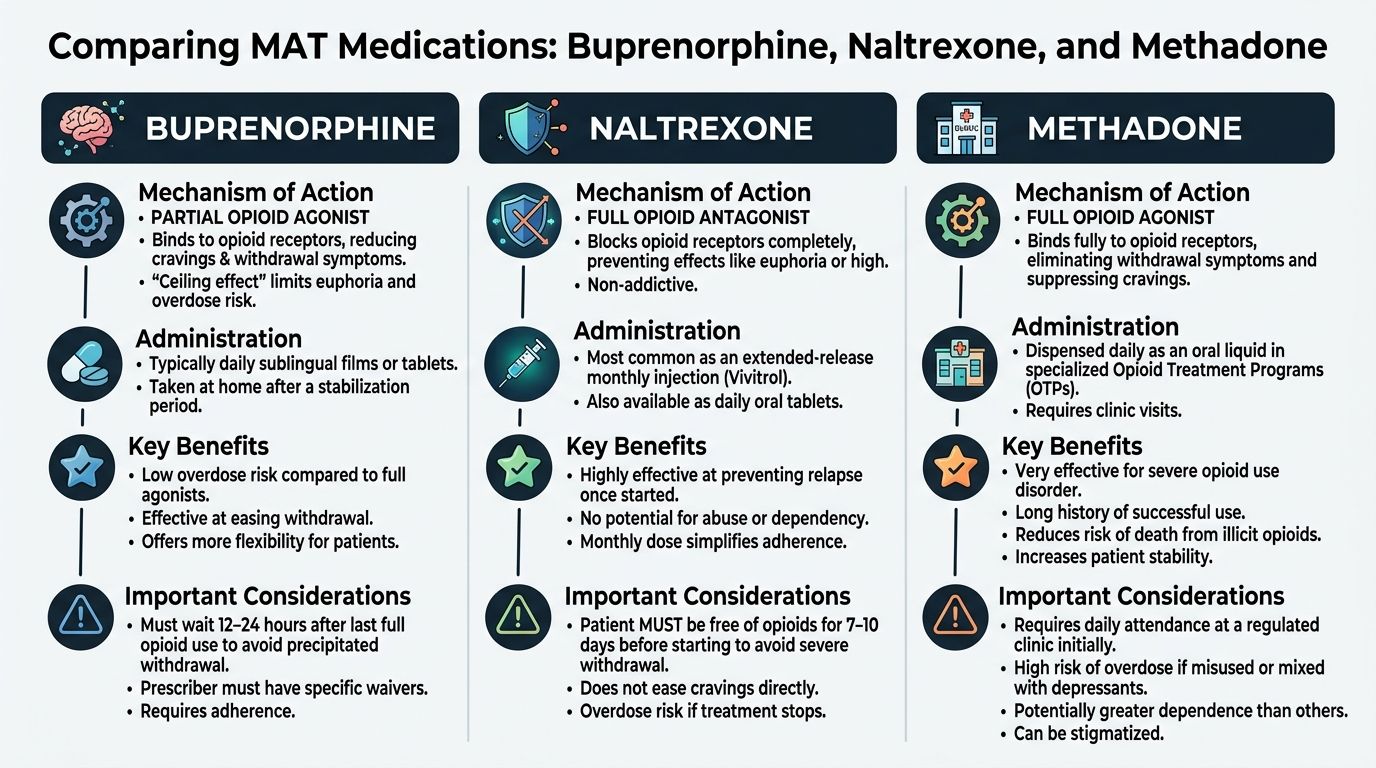
The three main medications used in medication assisted treatment for opioid addiction are not interchangeable in every case. Each one can be useful. Each one also comes with trade-offs in safety, flexibility, and fit.
Buprenorphine
Buprenorphine is a partial opioid agonist. In plain language, it activates opioid receptors enough to reduce withdrawal and cravings, but with less intensity than full agonists. It also helps block the effects of other narcotics.
For many patients, buprenorphine offers a practical balance of symptom relief and safety. It can help someone feel normal enough to work on recovery without producing the same cycle of intoxication and crash that drives addiction.
Its flexibility also matters. Buprenorphine can be prescribed in office-based settings, which is useful for patients who need privacy, travel flexibility, or a treatment path that can continue more discreetly after a higher level of care.
Methadone
Methadone is a full opioid agonist. It has long been used effectively in opioid treatment, especially for patients with more severe dependence or those who have not done well with other approaches.
Methadone can be highly effective, but the safety margins are tighter. Methadone has a narrow therapeutic window, and a lethal dose for opioid-naive individuals is reported at 70 to 75 mg, which creates a higher accidental overdose risk than buprenorphine according to the National Treatment Court Resource Center MAT guidance.
That same guidance also notes a practical difference many families overlook. Methadone generally requires daily dispensing through regulated opioid treatment programs. For some patients, that structure is helpful. For others, especially executives, parents, or public-facing professionals, it can make treatment continuity harder because it offers less mobility and less privacy.
Naltrexone
Naltrexone is an opioid antagonist. It works differently from methadone and buprenorphine because it blocks opioid receptors rather than activating them. That means it does not reduce withdrawal in the same way agonist medications do.
For the right patient, this can be appealing. It is a non-opioid option. But there is a practical challenge. A person must be fully off opioids before starting it, or the medication can trigger withdrawal. That makes induction harder for many people.
The durability of treatment can also differ. In the verified data, naltrexone showed a shorter mean treatment duration than buprenorphine or methadone. In real clinical planning, that matters because shorter retention usually means a rougher path to stability.
How clinicians decide
Medication choice is not a popularity contest. It is a matching process. A clinician looks at opioid history, current use pattern, overdose risk, treatment setting, co-occurring mental health conditions, patient preference, and how much daily structure is needed.
Some patients need the high level of structure built around methadone. Some are better served by buprenorphine because it is safer and easier to continue privately after discharge. Some can do well with naltrexone if they are already through detox and strongly prefer an antagonist approach.
The best medication is the one a patient can start safely, tolerate well, and stay engaged with over time.
Comparison of MAT Medications for Opioid Addiction
| Medication | How It Works (Mechanism) | Administration Method | Key Benefit |
|---|---|---|---|
| Buprenorphine | Partial opioid agonist that reduces cravings and withdrawal while helping block other narcotics | Office-based prescribing can support flexible continuation of care | Strong safety profile with more privacy and flexibility |
| Naltrexone | Opioid antagonist that blocks opioid receptors | Taken after a patient is fully off opioids | Non-opioid option for selected patients |
| Methadone | Full opioid agonist that reduces withdrawal and cravings through sustained receptor activation | Daily dispensing through regulated opioid treatment settings | Can be effective for severe or long-standing opioid dependence |
A practical takeaway for families
Families often want to know which medication is strongest. A better question is which medication is most sustainable for this person in this phase of treatment. Opioid care works better when the plan fits the patient’s medical needs and real life constraints, not when it follows a rigid ideology.
How to Access MAT and Understand Your Coverage
The most effective use of medication assisted treatment for opioid addiction happens inside a continuum, not in isolation. Medication helps a person become stable. The rest of treatment helps that person stay well.
Detox is the starting point, not the endpoint
Many patients arrive in treatment in a physically brittle state. They are sleep deprived, dehydrated, anxious, and afraid of withdrawal. In detox, medication can reduce the sharp edges of that crisis. That is often the first moment a patient feels relief instead of dread.
Once the body settles, the work changes. The goal is no longer just getting through the next hour. It becomes understanding the addiction pattern, the relapse history, the psychiatric symptoms, and the life pressures that kept opioid use in place. A closer look at the treatment arc appears in this overview of the detox and rehab process in a luxury rehab.
Therapy works better when the patient can engage
A patient in untreated withdrawal is usually not in a condition to process trauma, tolerate group work, or have productive family sessions. Medication can make those next steps possible.
That is one reason integrated care consistently matters. Research confirms that treatment retention requires not only appropriate pharmacotherapy but also integrated psychosocial and medical services, and patients receiving regular, frequent integrated services alongside opioid pharmacotherapy achieve superior outcomes compared with medication-only approaches as described by the ASPE report on retention and continuity of care.
The same report notes that proper medication dosing is very important for treatment retention. This is not a minor technical detail. If the dose is too low, cravings and withdrawal can break through. If the plan is poorly coordinated, patients disengage. Good MAT requires active adjustment, observation, and follow-up.
What integrated treatment often includes
Medical monitoring
Clinicians watch withdrawal symptoms, side effects, sleep, appetite, and other changes that affect early stability.Individual therapy
Many patients begin addressing grief, trauma, shame, perfectionism, or stress patterns that fuel opioid use.Family involvement
Families need guidance too. They often need help shifting from crisis management to healthy support.Step-down planning
Medication should continue smoothly from detox into residential, outpatient, and aftercare when clinically appropriate.
A medication can open the door to recovery. Ongoing therapy and medical coordination help keep that door open.
What does not work well
Two patterns tend to cause problems. The first is detox without a longer-term plan. Patients may leave physically improved but still vulnerable, with cravings and life stress waiting for them outside. The second is medication without enough clinical support. Some patients can do well with a lighter therapy schedule, but most need coordinated care, especially early on.
A strong program treats MAT as a foundation. It does not stop there.
MAT at Oceans Luxury Rehab A Premier California Program
For patients who need a private, medically supervised setting, the treatment environment can shape whether they enter care at all. Many professionals and families are not only looking for MAT. They are looking for a setting where opioid treatment can happen with dignity, confidentiality, and close clinical oversight.
Oceans Luxury Rehab provides medication assisted treatment as part of a broader continuum that includes medically supervised detox, residential care, outpatient treatment, dual-diagnosis support, physician oversight, nursing care, and aftercare planning. Program details are available on its medication assisted treatment page.
Why the setting matters
Opioid treatment is easier to accept when the environment lowers resistance instead of adding to it. A person who feels exposed, rushed, or overwhelmed may leave before stabilization occurs. A person who feels physically safe and respected is more likely to stay long enough for treatment to begin working.
That matters for professionals in California who may be balancing public visibility, family obligations, licensing concerns, or executive responsibilities. In those situations, privacy is not a luxury add-on. It is often the condition that makes treatment possible.
How luxury care supports MAT
A high-comfort setting does not replace evidence-based care. It supports it.
Private rooms can improve rest during early recovery. Round-the-clock nursing and physician involvement help with medication initiation, symptom monitoring, and dose adjustments. A calmer setting can also reduce the sensory overload many patients experience during withdrawal and early stabilization.
This model is especially useful for patients with co-occurring mental health conditions. Someone with opioid dependence and severe anxiety, depression, trauma symptoms, or burnout often needs psychiatric and addiction care moving in the same direction. When those services are integrated, the patient is not forced to choose which crisis gets treated first.
What families should look for in any California MAT program
The strongest programs usually share several traits:
Medical capability
MAT should be initiated and monitored by clinicians who understand withdrawal, dosing, safety, and psychiatric overlap.Continuity of care
The program should have a realistic plan for what happens after detox or residential treatment.Flexible therapy design
Patients need counseling and support, but the schedule should match clinical need rather than forcing a one-size-fits-all format.Confidentiality and comfort
Patients who need discreet care are more likely to engage when the setting protects privacy.
A luxury treatment center is not defined by decor alone. In opioid care, the primary value is coordinated medicine, therapy, privacy, and a setting where a patient can stay focused long enough for recovery to take hold.
How to Access MAT and Understand Your Coverage
Starting medication assisted treatment for opioid addiction is often easier once the process is broken into a few concrete steps. Most patients do not need more motivation. They need a clear path.
The first steps
Schedule a confidential assessment
A clinical team needs to know what opioids are being used, how recently, whether there have been overdoses, and whether there are co-occurring psychiatric or medical issues.Confirm the right level of care
Some patients need detox first. Others may be able to start at a residential or outpatient level, depending on withdrawal risk and stability.Discuss medication fit
The treatment team should explain whether buprenorphine, methadone, or naltrexone makes sense based on current opioid use and treatment goals.Build a continuity plan
Before treatment starts, it helps to know how medication follow-up, therapy, and step-down care will be handled.
Insurance questions families should ask
Many people delay care because they assume insurance will be confusing or that MAT will not be covered. Coverage depends on the plan and the level of care, but verification is usually straightforward when an admissions team handles it directly.
Questions to ask include:
What level of care is covered
Detox, residential treatment, partial hospitalization, and outpatient benefits may differ.How medication services are billed
Families should ask how physician visits, psychiatric care, and medication management fit into benefits.What the out-of-pocket responsibility may be
It helps to clarify deductibles, copays, and any authorization requirements early.
A practical overview of common coverage issues appears in this article on whether insurance covers drug rehab.
When a patient is ready, speed matters. Delays create room for second thoughts, worsening withdrawal, and relapse risk.
What to expect from admissions
A strong admissions process should be calm, discreet, and clinically informed. Patients and families should come away understanding the immediate next step, what to bring, who will evaluate medication needs, and how privacy will be protected.
The goal is not to master every insurance detail before reaching out. The goal is to get a clinical conversation started quickly and let the treatment team help sort out the logistics.
Common Questions About Medication Assisted Treatment
Families often reach the point of understanding MAT intellectually but still carry emotional doubts about it. Those concerns deserve direct answers.
Is MAT just replacing one addiction with another
No. Properly prescribed MAT is a medical treatment for opioid use disorder. The aim is not intoxication. The aim is to reduce cravings, prevent withdrawal, lower relapse risk, and support stable functioning so the person can participate in recovery.
A patient taking medication on a structured plan under supervision is in a very different clinical situation than a person compulsively using illicit opioids despite harm.
Does everyone on MAT need therapy
Therapy is strongly recommended, but the exact amount and format should fit the individual.
Clinical guidelines recommend combining MAT with counseling, yet studies show mixed evidence on whether every patient needs the same level of psychosocial treatment. A small percentage of people with opioid use disorder receive any MAT prescription, and this uncertainty is one reason individualized programs are important according to the Illinois Criminal Justice Information Authority overview of MAT.
That does not mean therapy is optional in any broad sense. It means treatment should be individualized. A patient with trauma, severe depression, family conflict, or repeated relapse usually needs a richer therapy structure than someone who is medically stable and doing well with focused follow-up.
How long does someone stay on medication
There is no single timeline that fits every patient. Some need medication for a shorter period. Others do better with longer maintenance. The safer approach is not to rush tapering for ideological reasons.
Clinicians usually focus on stability first. If a patient is sleeping well, functioning, engaged in therapy, avoiding illicit opioid use, and building a stable life, those are signs of progress. Decisions about tapering should come later and should be made carefully.
What if a patient wants privacy
That is a legitimate concern, especially for executives, licensed professionals, and families in tight social circles. Privacy can influence whether a person seeks care early or waits until the situation worsens.
This is one reason office-based options such as buprenorphine can be valuable for some patients, and why discreet residential settings can improve engagement during the early phase of treatment.
Can MAT work for someone with depression, anxiety, or trauma too
Yes, but only if the program recognizes that addiction and mental health symptoms often reinforce each other. Opioid use may begin as a way to numb anxiety, grief, insomnia, or trauma symptoms. If those issues are ignored, relapse risk stays high even when detox goes well.

What should families remember most
Medication assisted treatment for opioid addiction is not surrender. It is treatment. It gives people a real chance to step out of the cycle of craving, withdrawal, secrecy, and fear.
The right plan is rarely the most rigid one. It is the one that is safe, individualized, and sustainable.
If opioid use has started to take over daily life, Oceans Luxury Rehab offers confidential support for people exploring treatment options in California. The admissions team can help arrange an assessment, discuss whether medication assisted treatment is clinically appropriate, and review insurance benefits so the next step feels clear and manageable.