
A lot of families reach this topic after a rough night. Someone used an aerosol, a solvent, or another inhaled chemical for what looked like a short escape. Then they stopped and expected the problem to fade. Instead, the body started reacting. Sweat, shaking, nausea, panic, cravings, confusion. In some cases, the fear comes from one simple question: can stopping inhalants be dangerous?
It can.
That surprises people because inhalants are often misunderstood as a “less serious” drug problem. They’re common household or industrial products, not something sold in a typical street-drug transaction. That familiarity lowers people’s guard. It also delays treatment.
The Unseen Crisis of Inhalant Withdrawal
A common pattern looks like this. An adult starts using compressed gas, spray products, or solvents in private because they seem easy to hide and easy to get. There’s no needle, no pill bottle, no obvious paraphernalia. The person tells themselves it’s not the same as alcohol, opioids, or cocaine. Then they try to stop and find out their brain and body have adapted more than they realized.
Withdrawal from inhalants can be physically painful, psychologically destabilizing, and medically risky. Some people develop headaches, nausea, sweating, tremors, agitation, and intense anxiety. Others face more severe neurological symptoms, including hallucinations or convulsions. That’s why inhalants withdrawal symptoms should never be brushed off as a minor rebound or simple irritability.
What makes this crisis easy to miss is the packaging. Glue, sprays, fuels, cleaners, and gases don’t look like “hard drugs.” But the nervous system doesn’t care what aisle the product came from. It only responds to repeated chemical exposure and then reacts when that exposure suddenly stops.
Inhalant withdrawal isn’t just emotional discomfort. In some people, it becomes a medical event.
That’s the line families need to understand early. Waiting for things to “settle down” at home can turn a treatable withdrawal syndrome into an emergency. A safer approach starts with recognizing what inhalants are, what they do to the brain, and why stopping them can trigger such a volatile response.
Understanding What Inhalants Are
Inhalants are substances people breathe in to change how they feel. The category is broad, and that’s part of the danger. These aren’t one drug with one formulation. They’re a range of chemical products that can depress the central nervous system or otherwise alter perception and sensation.

The main categories people should know
Most inhalants fall into four practical groups:
- Volatile solvents include products such as paint thinners, glue, and cleaning or degreasing fluids.
- Aerosols include spray paints, deodorant sprays, and other pressurized products.
- Gases include butane products, refrigerant-type gases, and nitrous oxide from whipped cream dispensers or similar sources.
- Nitrites are often referred to as poppers and act differently from many other inhalants, but they’re still part of the broader category.
The common thread is access. Many of these products sit in garages, bathrooms, kitchens, cars, or workplaces. They’re legal to own for their intended use, which creates a false sense of safety when they’re misused.
Why they affect the brain so fast
When someone inhales these chemicals, they reach the bloodstream quickly through the lungs and then hit the brain rapidly. That speed is part of what reinforces use. The effect may feel immediate, but so is the physiological disruption. Repeated exposure can alter how the brain regulates mood, attention, arousal, and reward.
A simple analogy helps. Inhalants act like flooding an electrical panel with the wrong current. At first, lights flicker in a way the user interprets as a “high.” Over time, the wiring becomes unstable. When the current is cut off, the system doesn’t just return to normal. It can surge, misfire, and shut down irregularly.
Historical research supports that dependence can become physical, not just psychological. A classic animal study found that mice exposed to the solvent TCE for four days developed convulsions when exposure stopped, and those convulsions eased within 30 to 60 minutes after re-exposure to TCE or toluene, according to research on inhalant dependence and withdrawal.
Why this matters for families
The phrase “just household products” is one of the most dangerous misunderstandings in addiction care. The brain doesn’t treat repeated solvent or gas exposure as harmless because the label came from a hardware store or kitchen cabinet.
That’s why clinicians take inhalants withdrawal symptoms seriously. The category may look ordinary on a shelf. The withdrawal picture can look anything but ordinary in real life.
Recognizing Common and Severe Withdrawal Symptoms
The symptom picture usually isn’t limited to one system. Inhalants withdrawal symptoms often hit the body, the mind, and the nervous system at the same time. That overlap is what makes the experience so destabilizing. A person may feel sick, frightened, unable to sleep, mentally foggy, and overwhelmed by cravings all within the same day.
A major population study found that inhalant withdrawal is not rare. About 47.8% of people with inhalant dependence experienced three or more clinically significant withdrawal symptoms, with a prevalence nearly identical to cocaine withdrawal, according to the NESARC-based study on inhalant withdrawal.
The common physical symptoms
The early physical phase can feel like the body is revolting. Common symptoms include:
- Headaches that range from dull pressure to pounding discomfort
- Nausea and vomiting that make hydration difficult
- Excessive sweating and chills that come in waves
- Tremors or visible shakiness, especially in the hands
- Runny eyes or nose that can be mistaken for illness
- Abdominal cramps and general physical agitation
These symptoms can look less dramatic than other forms of withdrawal at first glance, but they matter. They can wear a person down quickly, interfere with eating and sleeping, and increase the urge to use again to make the discomfort stop.
The severe neurological symptoms
Such underestimation becomes dangerous. In more serious cases, withdrawal can involve:
- Hallucinations
- Disorientation
- Agitation that escalates rapidly
- Convulsions or seizures
The best analogy is a city power grid after repeated surges. Signals stop traveling smoothly. Some circuits go dark, others overload, and nothing is coordinated. In a human brain, that can translate into abrupt shifts in awareness, sensory distortion, and dangerous neurological instability.
Practical rule: If a person stopping inhalants becomes confused, starts seeing or hearing things, or shows seizure-like activity, that’s an emergency, not a wait-and-see situation.
The psychological symptoms that often drive relapse
Families often focus on visible symptoms and miss the psychological pressure building underneath them. That pressure is one reason people return to use even when they desperately want to stop.
Psychological symptoms may include:
- Intense cravings
- Anxiety
- Irritability
- Depressed mood
- Insomnia
- Poor concentration
- Restlessness
These symptoms can feel less urgent than convulsions, but they’re central to treatment. A person may think, “The worst is over,” once the sweating or nausea eases. Then the emotional crash arrives. Sleep gets fragmented. Mood becomes unstable. Attention narrows to one thought: use something to get relief.
That’s why a good withdrawal response doesn’t just monitor vital signs. It also watches for the mental and emotional shifts that put recovery at risk. Families who want a broader view of body warning signs during detox can review this guide on symptoms of detoxing and when to pay attention.
When symptoms stop being manageable at home
Home detox becomes a gamble when symptoms are changing hour by hour. A person may start with nausea and agitation, then move into confusion, panic, or severe sleep loss. Once that pattern develops, judgment falls off. The person withdrawing may minimize what’s happening, resist help, or become too impaired to ask for it.
That’s why inhalants withdrawal symptoms deserve the same clinical seriousness people already grant to other high-risk withdrawal states. The label on the product may be ordinary. The withdrawal response may be anything but.
The Inhalant Withdrawal Timeline Explained
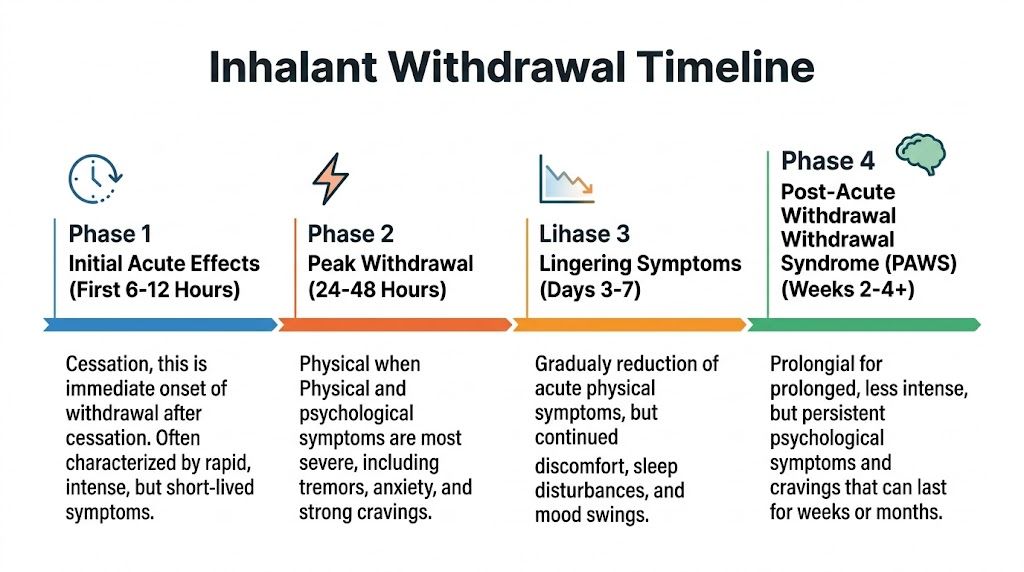
Families often ask one practical question first: how long does this last? The most accurate answer is that inhalant withdrawal often follows a biphasic pattern. The early period leans more physical. The later period shifts toward psychological and cognitive distress.
According to clinical guidance on inhalant withdrawal timelines, acute physical symptoms such as sweating, tremors, and nausea can begin within hours to 2 days, peak within 2 to 5 days, and then give way to psychological symptoms like cravings, anxiety, and mood changes that can last 7 days or more.
Early phase and peak distress
The first stretch is the most unpredictable. Symptoms may start within hours or may become more obvious over the next day or two. During this window, the body is reacting to the abrupt absence of chemicals it had adapted to.
Physical symptoms often dominate here. Sweat, tremor, nausea, headaches, cramps, and agitation can all appear. In more severe cases, neurological symptoms can emerge during this same period, which is why close monitoring matters most early on.
The shift into psychological withdrawal
After the acute physical phase begins to settle, many people expect to feel substantially better. That expectation can backfire. The body may look calmer while the mind becomes harder to manage.
Anxiety can stay high. Cravings may intensify. Sleep often remains poor. Mood can swing from irritability to flatness to despair. Concentration can remain weak, which makes ordinary tasks feel surprisingly hard.
The most deceptive stage is often the one after the visible physical symptoms ease. That’s when people assume they’re safe and underestimate relapse risk.
A practical view of the timeline
The table below gives a simple reference point. Individual cases vary, especially when a person has used multiple substances or has co-occurring mental health symptoms.
| Phase | Typical Duration | Common Symptoms |
|---|---|---|
| Initial onset | Within hours to 2 days | Headaches, nausea, sweating, chills, agitation, early cravings |
| Peak physical withdrawal | 2 to 5 days | Tremors, vomiting, cramps, insomnia, severe anxiety, possible neurological complications |
| Psychological transition | 3 to 7 days | Irritability, depression, poor concentration, strong cravings, disturbed sleep |
| Ongoing post-acute effects | 7 days or more | Mood changes, anxiety, cravings, cognitive fog, relapse vulnerability |
Why the timeline matters clinically
A timeline isn’t just for setting expectations. It changes care decisions.
If a person is still in the early physical phase, medical staff focus on safety, hydration, symptom stabilization, and watching for dangerous escalation. If the person has moved into the psychological phase, treatment has to address cravings, insomnia, anxiety, and the emotional crash that often drives return to use.
A family trying to manage this at home often assumes progress is linear. It usually isn’t. Withdrawal can improve in one domain while worsening in another. That uneven pattern is one reason professional detox remains the safer route.
Why Medically Supervised Detox Is Not Optional
With inhalants, the central problem isn’t just discomfort. It’s unpredictability. A person can look “mostly okay” and still be at risk for rapid deterioration. That’s why supervised detox should be treated as a medical necessity, not a luxury.

A study on diagnostic validity found a strong graded relationship between severity of use and withdrawal symptoms. 77.3% of individuals with inhalant dependence reported at least one withdrawal symptom, compared with 12.2% of non-disordered users, according to research examining inhalant withdrawal severity. That kind of pattern tells clinicians something important. Risk rises with dependence, and outward appearances don’t reliably show where someone falls on that spectrum.
What medical detox actually does
Medical detox protects the patient in ways home withdrawal can’t. Staff can monitor changing symptoms, identify warning signs early, and intervene before a manageable problem becomes a crisis.
That usually includes:
- Continuous observation for agitation, confusion, hallucinations, or seizure activity
- Supportive medical care for nausea, dehydration, sleep disruption, and severe anxiety
- Rapid escalation protocols if neurological symptoms emerge
- Assessment for co-occurring disorders that complicate the withdrawal picture
The most important trade-off is simple. Home detox may feel private and easier to start. It also removes the safety net when symptoms turn severe. Clinical detox asks the patient to accept monitoring and structure, but in exchange it lowers the chance of catastrophic complications.
What doesn’t work
Several home strategies fail repeatedly.
- White-knuckling through it ignores the seizure and psychosis risk.
- Using other substances to “take the edge off” can complicate the withdrawal picture and mask deterioration.
- Waiting for the person to ask for help often means waiting until judgment is impaired.
A person in withdrawal is not always in a condition to accurately judge how sick they are.
For California families looking at next steps, reviewing the standards of a proper detox center in California can help clarify what supervised care should include.
Why the first decision matters so much
The first treatment setting shapes everything that follows. If detox is chaotic, interrupted, or medically thin, the patient starts recovery from a place of exhaustion and instability. If detox is structured and closely supervised, the patient has a better chance of moving into therapy with a clear mind and a stronger physical footing.
That’s why this stage should never be approached as a test of willpower. It’s a medical stabilization process.
Evidence-Based Treatments for Lasting Recovery
A patient can clear inhalants from the body and still be in real danger of relapse a few days later. I see this mistake often. Families assume the crisis has passed because the substance is gone, while the patient is still dealing with panic, insomnia, depression, irritability, trauma cues, and the habits that made inhalant use feel like relief.
That is why treatment after detox has to be organized with the same seriousness we bring to alcohol or opioid recovery. Inhalant addiction is often minimized because the products are common and cheap. The brain and nervous system do not treat it as minor.
Dual-diagnosis care improves the odds
Inhalant use rarely exists in isolation. Anxiety, depression, trauma symptoms, poor sleep, attention problems, and unstable mood often sit right beside it. If those problems are left untreated, the patient leaves rehab carrying the same internal pressure that fed the addiction in the first place.
Care works better when addiction treatment and mental health treatment are built into one plan. If cravings spike after a conflict at home or after a trauma reminder, the response should be immediate and coordinated, not split between disconnected providers.
A useful framework is trauma-informed care. In practice, that means creating safety, predictability, and trust, while avoiding the kind of shaming or aggressive confrontation that can push a vulnerable patient back toward use.
Therapies that actually change behavior
No single therapy fixes inhalant addiction. Recovery usually improves through repetition, structure, and learning new responses under stress.
The core approaches often include:
- Cognitive behavioral therapy to identify the beliefs and thought patterns that drive use, such as “I can’t settle down without this” or “one slip won’t matter.”
- Dialectical behavior therapy to build distress tolerance, impulse control, and emotional regulation.
- Individual therapy to address shame, secrecy, trauma, grief, and the personal triggers tied to relapse.
- Group therapy to reduce isolation and let patients practice honesty, accountability, and coping skills with other people.
- Family therapy or family education to repair communication, set boundaries, and reduce enabling patterns at home.
These therapies matter because inhalant addiction usually becomes a fast reflex. Stress rises, access is easy, and use follows before the person has fully thought it through. Treatment has to slow that sequence down and replace it with something safer.
Medication has a limited but real role
There is no FDA-approved medication designed specifically for inhalant withdrawal or inhalant use disorder. That does not mean medication has no place in care.
In selected cases, physicians may use medications to target agitation, sleep disruption, mood symptoms, or co-occurring psychiatric conditions. The trade-off is straightforward. Medication can stabilize a patient enough to participate in therapy, but it also requires careful monitoring, especially when there are cardiac concerns, neurological symptoms, or other psychiatric prescriptions in the picture.
Good programs do not force every patient into the same formula. They use medication selectively, with clear goals and close follow-up.
The treatment plan should fit the person, not the facility
A teenager hiding aerosol cans in the garage needs a different plan than an adult with trauma history, repeated relapse, and severe insomnia. One patient may need strong psychiatric support. Another may need family boundary work and a tightly structured daily schedule. Another may need a longer residential stay because the home environment is saturated with triggers.
That is why individualized planning matters. This guide to individualized treatment plans in addiction recovery shows what that process should include.
Oceans Luxury Rehab is one California option that offers physician oversight, medically supervised detox, residential treatment, dual-diagnosis care, and step-down support. The point is not the name. The point is choosing a setting that can carry the patient from medical stabilization into real rehabilitation without gaps in care.
Recovery holds when treatment addresses both the substance use and the life conditions that keep pulling the person back to it.
Choosing High-Quality Inpatient Rehab in California
Not every person using inhalants needs the same level of care. Some can stabilize and move into a structured outpatient program. Others need the containment and medical visibility of inpatient treatment. The choice should depend on symptom severity, relapse risk, psychiatric complexity, home stability, and whether the person can remain safe outside a monitored setting.
When inpatient care makes the most sense
Inpatient or residential rehab is often the strongest fit when any of the following are present:
- Unstable withdrawal symptoms such as severe agitation, hallucinations, or seizure concern
- Repeated relapse after attempts to quit at home
- Co-occurring anxiety, depression, trauma symptoms, or other psychiatric issues
- A home environment with triggers, secrecy, or easy access to inhalants
- Poor sleep, weak nutrition, and overall physical depletion
For inhalant addiction, inpatient care does something outpatient treatment often can’t do at the start. It removes the person from the exact environment where the substance is hidden, normalized, and immediately available.
What to look for in a California program
A high-quality program should offer more than a bed and a therapy schedule. Families should look closely at the treatment mechanics.
Key markers include:
- Medical capability to manage withdrawal safely
- Psychiatric support for dual-diagnosis cases
- A full continuum of care so the patient can step down gradually instead of leaving treatment abruptly
- Privacy and discretion for professionals, executives, and public-facing clients
- Comfort that supports engagement, not comfort used as a substitute for real clinical depth
California patients often care about privacy for good reason. Many are balancing treatment with professional reputations, family roles, or public visibility. A discreet setting can reduce resistance to admission and help patients focus.
Why environment and structure both matter
A calm environment isn’t superficial when someone is withdrawing and trying to stabilize. Noise, crowding, and constant stress can make anxiety, cravings, and insomnia harder to manage. Private rooms, clinical consistency, and a lower-stimulus setting can support sleep, trust, and participation in therapy.
That said, comfort alone doesn’t produce recovery. The setting needs real structure. Patients need assessment, symptom monitoring, skilled therapy, relapse-prevention work, and a step-down plan that keeps support in place after inpatient care ends.
For many adults in Orange County and Los Angeles, the strongest inpatient option is the one that combines discretion, medical supervision, dual-diagnosis treatment, and a clear path into PHP, IOP, and outpatient care. In severe inhalant cases, that continuity often matters more than any single amenity.
Your Path to Healing Starts Today
Inhalants withdrawal symptoms can look deceptively simple at first and then turn serious fast. That’s why delay is risky. The person struggling may be ashamed, defensive, or convinced they should be able to stop without help. None of that changes the medical reality.
The safer response is straightforward. Treat inhalant withdrawal as a legitimate detox issue. Get a proper assessment. Use medical supervision when symptoms are active or severe. Follow detox with treatment that addresses cravings, mental health, behavior patterns, and the environment that kept the addiction going.
Recovery is possible. It usually starts when the family stops minimizing the substance because of where it came from, and starts responding to what it’s doing to the brain and body.
The next step doesn’t need to be perfect. It needs to be prompt.
If inhalant use has turned into withdrawal symptoms, panic, secrecy, or repeated failed attempts to quit, Oceans Luxury Rehab offers confidential admissions, medically supervised detox, residential treatment, and ongoing levels of care in San Clemente for adults in Orange County, Los Angeles, and across California. Speaking with admissions can clarify whether the current symptoms call for immediate detox and what level of treatment fits best.