
A senior manager walks into the office and suddenly can't do what used to feel routine. Email notifications trigger a jolt of panic. A certain conference room feels impossible to enter. A direct report asks a normal question, and the manager snaps, then spends the rest of the day ashamed and distracted. At night, sleep doesn't come easily. In the morning, the thought of work produces dread instead of momentum.
For high-functioning professionals, this can feel especially disorienting. Their identity may be built around control, judgment, resilience, and output. When concentration slips, memory falters, and ordinary interactions start to feel threatening, many assume they're burned out, weak, or merely failing to cope.
Sometimes that's not burnout. Sometimes it's PTSD from workplace exposure.
That phrase can sound too severe for an office, a hospital, a firm, a leadership team, or a corporate environment. But trauma at work doesn't always look like a dramatic accident. It can follow repeated intimidation, a violent incident, humiliating public mistreatment, harassment, discrimination, or being trapped in an environment that repeatedly overwhelms the nervous system. Once that happens, the mind and body can start reacting as if danger is still present, even when the workday looks normal from the outside.
When High Performance Gives Way to High Anxiety
One common pattern looks like this. A professional keeps performing after a disturbing workplace event because that's what they've always done. They show up to meetings. They hit deadlines. They tell themselves to move on.
Then the cracks appear.
They start rereading the same paragraph five times. They avoid one hallway, one team member, or one client account without fully admitting why. Their body stays tense all day, as if it's waiting for the next blowup, accusation, threat, or humiliation. Colleagues may see irritability. Family may see withdrawal. The person at the center of it often sees only one thing: a frightening loss of competence.
That confusion matters because workplace trauma is not rare or trivial. National Canadian compensation data shows PTSD-related lost-time claims rose from 1,207 in 2012 to 3,291 in 2022, nearly tripling over a decade, according to Canada's PTSD lost-time claims data. That trend doesn't diagnose any one person, but it does show that post-traumatic stress has become a meaningful force in working life.
Why high achievers often miss it
Professionals who are used to pushing through discomfort often mislabel trauma symptoms as performance problems.
- They call hypervigilance diligence. Constant scanning for risk can look like being thorough.
- They call avoidance strategy. Dodging a person, place, or task may get framed as efficiency.
- They call emotional numbing professionalism. Detachment may seem like composure.
- They call exhaustion normal. Chronic strain gets absorbed into a demanding career story.
Practical rule: If work feels dangerous long after the event, and the reaction shows up in the body as much as in thoughts, PTSD deserves consideration.
A successful career doesn't protect someone from trauma. In some cases, it hides the problem longer. The person keeps functioning just enough to delay help, while the internal cost rises.
Recognizing the Signs of Workplace PTSD
Symptoms of workplace PTSD usually make more sense when viewed through daily work behavior rather than textbook language. A professional may not identify with the term "intrusion," but they may understand what it means to freeze before opening a message from a certain executive, or to relive a confrontation during a client presentation.
A key point is timing. Symptoms may not fully show up on day one. A longitudinal study of medical workers exposed to violence found that PTSD symptoms, stress, and anxiety rose after exposure, peaked around one month, and then declined later, which is why the early post-incident period often matters so much for screening and support, as described in this study of symptom patterns after workplace violence.

Intrusion at work
Intrusion means the trauma keeps re-entering the day without permission.
A professional may experience:
- Unwanted memories during meetings, calls, or commutes
- Flashback-like moments when a raised voice, hallway, or Slack notification brings the event rushing back
- Nightmares that leave them exhausted before the workday starts
- Emotional flooding when reminded of a boss, department, or decision tied to the trauma
This isn't overthinking. It's the nervous system reacting as if the threat is present again.
Avoidance that looks like career management
Avoidance often gets mistaken for choice.
Someone may start:
- Skipping meetings where a triggering person will be present
- Delaying emails connected to the event
- Refusing projects that resemble the original trauma
- Working remotely whenever possible because the office itself feels unsafe
Avoidance can bring short-term relief. Over time, it can shrink a person's world and deepen the sense that work is unmanageable.
Changes in mood and thinking
This cluster often feels the most personal because it can alter a person's sense of self and career.
Common workplace versions include:
- Persistent self-blame such as "It was my fault" or "I should've handled it better"
- Loss of trust in leadership, colleagues, or the profession itself
- Emotional numbness during conversations that used to matter
- Cynicism and detachment that feel foreign to the person's usual values
A professional doesn't need to be having dramatic flashbacks every day for trauma to be shaping how they think, feel, and function at work.
Arousal and reactivity
This is the body staying on alert.
A person may notice:
- Trouble concentrating
- Irritability or anger
- Sleep disruption
- Being easily startled
- Feeling "on" all the time, even in low-risk settings
For high performers, this can be one of the most damaging parts. The mind becomes less available for judgment, creativity, diplomacy, and sustained attention, which are often the very skills their role demands.
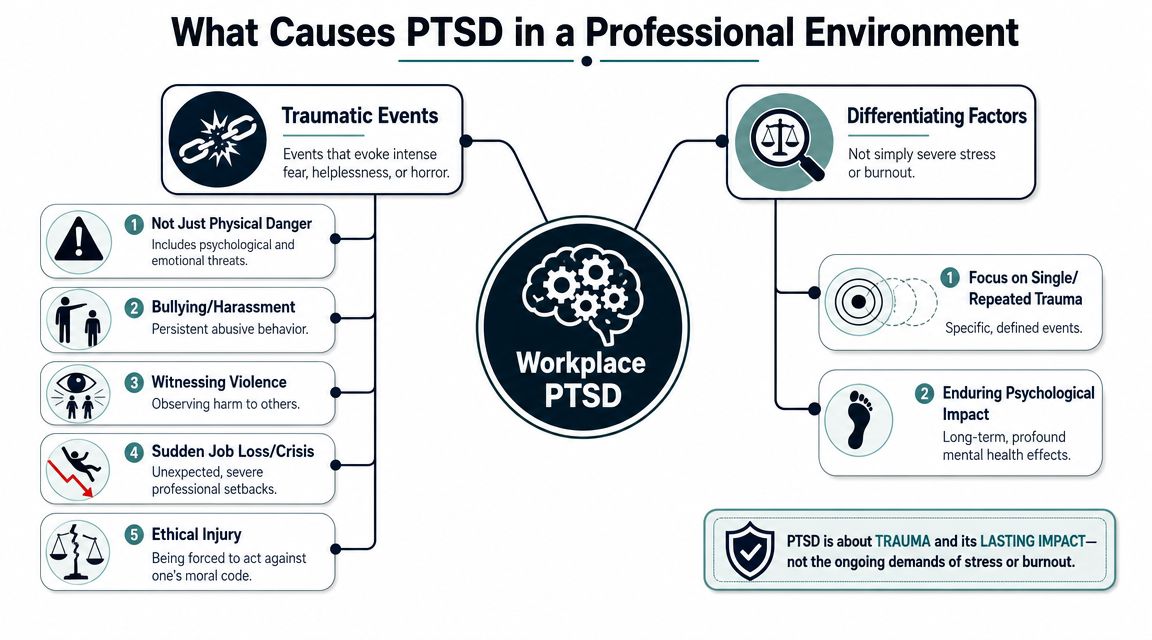
What Causes PTSD in a Professional Environment
Not every stressful job causes PTSD. Long hours, difficult clients, and pressure can produce burnout, anxiety, or depression without meeting the threshold for trauma. The difference is that PTSD usually grows from an experience, or repeated experiences, that overwhelm a person's sense of safety and leave a lasting fear-based response.
That can happen in visibly dangerous roles, but it can also happen in offices, hospitals, schools, legal settings, executive suites, and sales environments.
Workplace reporting cited by Workplace Options on workplace trauma and work-related PTSD notes that about 7% to 19% of workers who experience workplace trauma may develop PTSD, and the same source says employee PTSD risk has shown a 121% increase since 2020. That matters because it widens the picture beyond a narrow set of occupations.
What can be traumatic at work
A traumatic work environment may involve one event or repeated exposure.
Examples include:
- Violence or threats. An assault, stalking, credible threat, or witnessing harm to a coworker.
- Bullying by a superior. Repeated humiliation, intimidation, or public degradation that creates ongoing fear.
- Harassment or discrimination. Especially when a person feels trapped, powerless, and repeatedly targeted.
- Ethical injury. Pressure to act against firmly held moral standards in a way that leaves lasting psychological distress.
- Catastrophic professional crises. A severe event that leaves someone feeling terrified, helpless, or psychologically shattered.
Burnout versus trauma
Burnout often sounds like exhaustion, cynicism, and reduced effectiveness. Trauma usually carries a stronger fear response and more defined triggers.
A simple comparison helps:
| Pattern | Burnout | Workplace PTSD |
|---|---|---|
| Core experience | Overload and depletion | Threat, terror, helplessness, or violation |
| Triggers | General work demands | Specific reminders, people, places, or situations |
| Body response | Fatigue and disengagement | Hypervigilance, startle, panic, shutdown |
| Behavior | Pulling back from effort | Avoidance linked to trauma reminders |
For readers trying to understand legal and occupational implications, Scher, Bassett & Hames psychiatric injury guidance offers a useful overview of how psychiatric injuries can be framed in a workplace context.
If a person keeps asking, "Was it really bad enough?" that question itself is often part of the trauma response. Many professionals minimize what happened because acknowledging it would force a painful reassessment of their workplace, identity, or leadership environment.
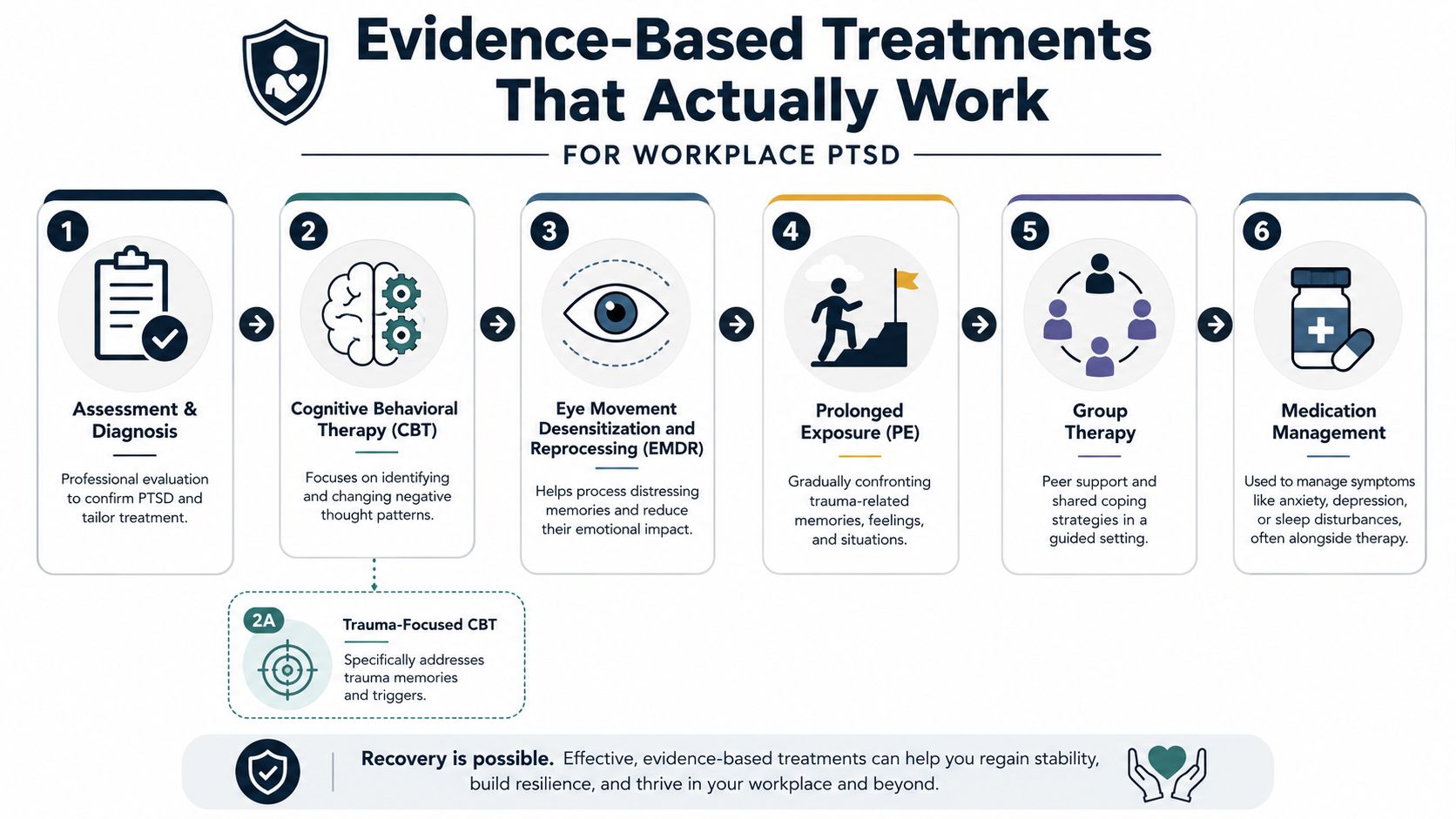
Evidence-Based Treatments That Actually Work
PTSD responds best to treatment that addresses trauma directly. General support helps, but many professionals become frustrated when standard talk therapy leaves the core reaction untouched. They may understand the event intellectually and still feel hijacked by reminders, panic, shame, sleep disruption, or avoidance.
That doesn't mean treatment has failed. It usually means the treatment needs to be more targeted.
What trauma-focused care aims to do
The goal isn't to erase memory. The goal is to reduce the nervous system's alarm response so the memory no longer runs the workday.
Occupational health reporting has noted that workplace markers such as reduced concentration, avoidance, absenteeism, and productivity loss often justify referral for specialized treatment and accommodations. In practice, those are often the signs that a professional needs formal trauma care rather than more willpower.
Helpful options commonly include:
- Trauma-focused CBT. This approach helps a person identify and test distorted beliefs linked to the trauma, such as exaggerated guilt, danger, or hopelessness.
- EMDR. This method helps process distressing memories so they carry less immediate emotional force.
- Prolonged Exposure. This treatment gradually reduces fear by helping the person face trauma-related memories and cues in a structured way.
- Medication management. Medication can help with sleep, anxiety, mood, or related symptoms, usually as support rather than a complete solution.
For readers who want a clear overview of how cognitive behavioral approaches are used in practice, this comprehensive Vancouver CBT resource gives a useful primer.
Why professionals often need a more tailored setting
Executives and other high-responsibility professionals often need treatment that accounts for privacy, scheduling pressure, and the practical consequences of cognitive impairment. They may also need help with co-occurring substance use, sleep problems, or depression.
In those cases, a setting that can address both mental health and substance use under one plan may be more practical than fragmented care. For example, Oceans Luxury Rehab's overview of mental health and substance abuse treatment describes integrated treatment models for people dealing with both conditions at once.
The Hidden Link Between Workplace Trauma and Substance Use
Many professionals with unresolved trauma don't set out to develop a substance problem. They try to get through the night. They try to shut off the replay. They try to sleep before a board meeting, a surgery, a court appearance, a client pitch, or another day in the same environment that now feels dangerous.
That's where alcohol, sedatives, stimulants, or other substances can enter the picture.
Why self-medication makes sense at first
Trauma symptoms are exhausting. Hypervigilance keeps the body activated. Intrusive memories break concentration. Sleep becomes fragile. A drink, a pill, or another substance may seem to offer something immediate that trauma treatment has not yet provided: relief.
In the short term, substances may appear to help with:
- Falling asleep
- Turning down anxiety
- Numbing shame or anger
- Getting through social or professional obligations
- Creating emotional distance from workplace reminders
The problem is that this strategy usually strengthens the cycle rather than solving it. The trauma remains active, and the person now has a second problem layered on top of the first.
Why dual diagnosis matters
When PTSD and substance use show up together, they usually need to be treated together. If treatment addresses only the drinking or drug use, the unprocessed trauma may continue driving cravings, relapse, or shutdown. If treatment addresses only trauma and ignores the substance pattern, the person's nervous system may still be relying on chemical relief to get through daily life.
That combination is often called a co-occurring disorder or dual diagnosis.
Recovery tends to move faster when care treats the reason a person is using, not just the use itself.
For a deeper look at that connection, Oceans Luxury Rehab's discussion of the impact of trauma on addiction explains how trauma symptoms and substance use can reinforce each other.
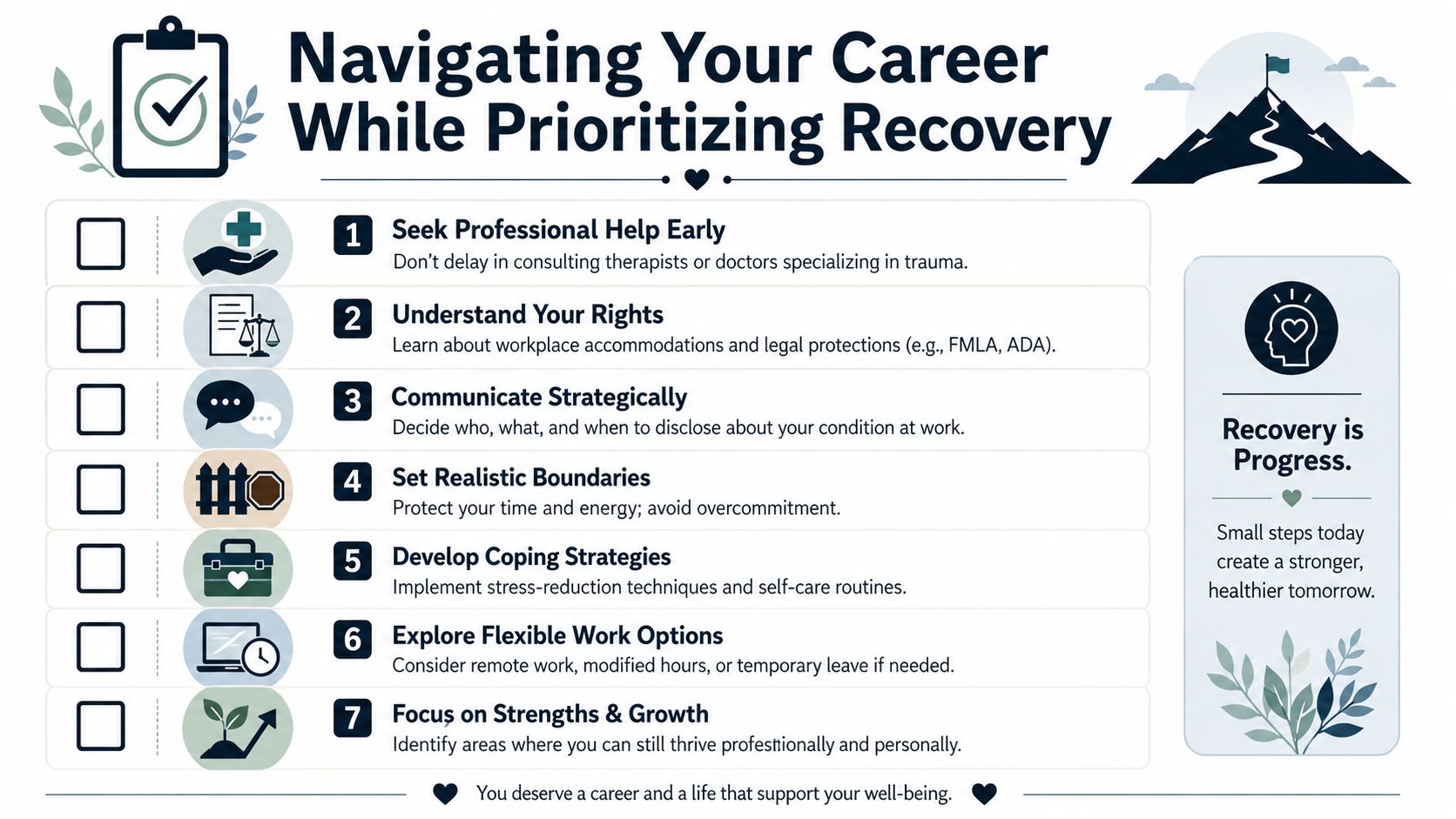
Navigating Your Career While Prioritizing Recovery
One of the biggest barriers to treatment is fear. A professional may worry that getting help will damage credibility, derail advancement, or permanently alter how colleagues see them. That fear is understandable, especially in environments that reward composure and punish visible struggle.
Still, protecting a career often starts with protecting health.
Research on workplace-specific interventions is encouraging. Studies of approaches such as on-site work evaluations and graded work exposure have reported return-to-work rates of 87% to 88% in included studies, according to this review of return-to-work interventions for PTSD. That doesn't guarantee a simple path, but it does support a practical point: career continuation and recovery can fit together.
A strategic approach to disclosure
Not everyone at work needs the full story.
A more useful framework is to decide:
- Who needs to know. Often that's limited to HR, a supervisor, or a designated occupational contact.
- What they need to know. Usually the focus should be on functional impact and needed support, not intimate details.
- When to say it. Earlier conversations are often easier than crisis-driven disclosure after a blowup or collapse.
A professional can often say, in effect, that a health condition is affecting concentration, sleep, or stress tolerance and that treatment is underway. Specific trauma content usually doesn't need to be shared unless the person wants to share it.
What accommodations may look like
Reasonable accommodations vary by role, setting, and employer, but common examples include:
- Modified schedule. Later start times, reduced hours for a period, or time for appointments.
- Work environment adjustments. A quieter workspace, remote work, or reduced exposure to triggering settings.
- Temporary task changes. Shifting away from certain meetings, accounts, or duties while treatment begins.
- Structured return plans. Gradual re-entry instead of an abrupt full-load comeback.
Boundaries that protect recovery
Many high performers try to prove they're still capable by overcommitting during early recovery. That usually backfires.
Helpful boundaries often include:
- Reducing optional stressors
- Limiting after-hours availability
- Building transition time before and after work
- Prioritizing treatment appointments
Work can be part of recovery when it restores structure and meaning. It becomes a threat when a person uses it to outrun symptoms that need treatment.
Choosing Discreet High-Quality Care in California
For professionals dealing with PTSD from workplace exposure, treatment isn't a luxury purchase. It's a strategic health decision with career implications. The setting matters when privacy, sleep, clinical quality, and the ability to address co-occurring substance use all affect whether someone completes care and stabilizes.
The right program usually has several features. It should offer trauma-informed assessment, strong dual-diagnosis capability, and a continuum of care that can adapt as symptoms improve. It should also respect confidentiality, because many professionals delay treatment less from denial than from concern about exposure.
In California, Oceans Luxury Rehab's DBT Center of Orange County resource is one entry point for understanding a treatment environment designed for people who need discreet, high-comfort care. Oceans Luxury Rehab is a licensed oceanfront center in San Clemente that provides detox, residential treatment, outpatient levels of care, dual-diagnosis support, physician oversight, and private rooms. For a professional whose trauma symptoms have become entangled with alcohol or drug use, that kind of integrated structure can make treatment more workable.
The practical question isn't whether a successful person should need this level of support. The practical question is what gives recovery the best chance to hold. When work identity is strong, treatment should help preserve function, judgment, and long-term stability, not just relieve symptoms for a week.
For professionals in Orange County, Los Angeles, and across California who need confidential help for trauma, substance use, or both, Oceans Luxury Rehab offers a discreet path forward with private accommodations, evidence-based care, and treatment options that can support recovery without losing sight of career realities.